
Almost 50% of the patients started their journey at near-end-of-life with progressive and life-threatening failure of the digestive system (liver) or the kidneys and followed the body’s natural path toward death in an orderly and predictable manner as I had illustrated on my Hierarchy of the Body card.
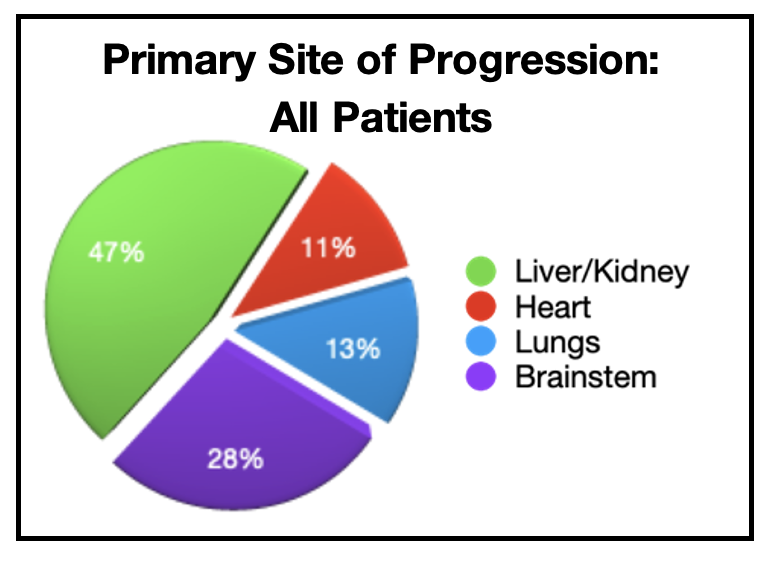
However, just over 50% of the patients began their near-end-of-life journey with a life-threatening assault to the other essential organs, heart, lungs and brainstem, before they had any compromise of their digestive system and their kidneys. I knew that, in significant ways, these patients would not follow the natural path toward death. The heart, lungs and brainstem were much more important to survival and their functions were so intimately interrelated that the failure of one would quickly lead to the failure of the other two.
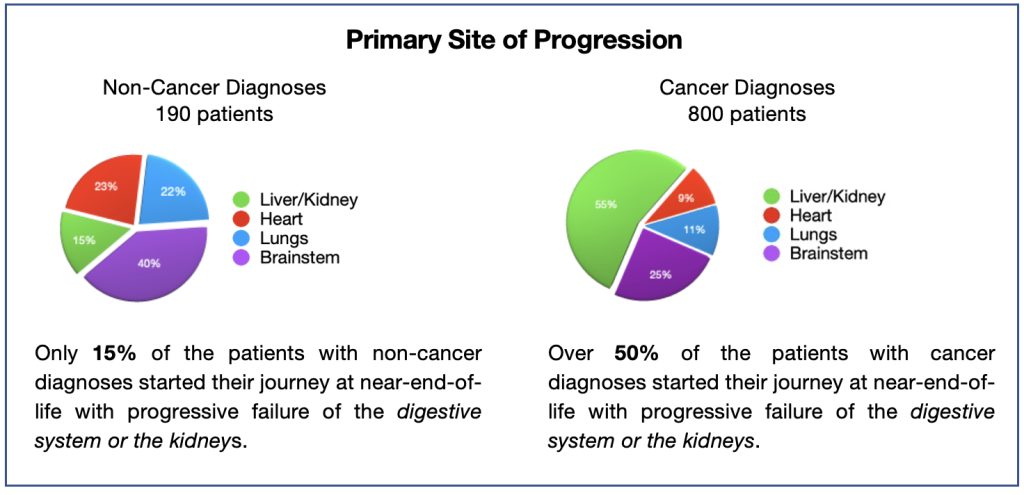
Primary Site of Progression Sorted by Non-Cancer and Cancer Categories:
I still had my clinical intuition telling me that the near-end-of-life journeys of patients with non-cancer and cancer diagnoses were very different. Based on that feeling, I decided to continue my review using the data of the patients within each ‘category’ separately to determine if there were differences in their primary site of progression.
Using this approach, I quickly verified my clinical experience – the journeys toward death of patients with non-cancer diagnosis were likely to be significantly different from the journeys of patients with cancer diagnoses. The pie charts below illustrate the scientific basis of these major differences.
Now, my review needed to focus on the effect that these different life-threatening ‘triggers’ had on body’s path toward death. My findings from the data demonstrated that:
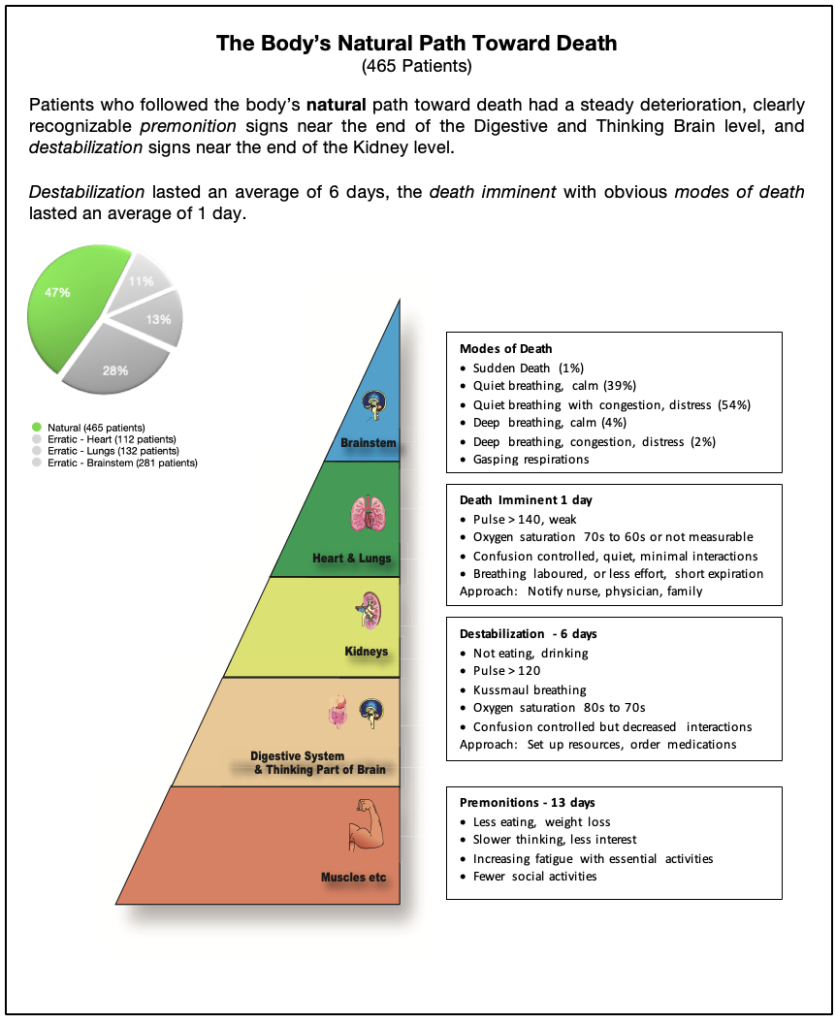
The patients whose life-threatening event was failure of the liver or the kidneys, followed the body’s natural path toward death under the brainstem’s control of the essential organs shutting down in an orderly, sequential manner as I had illustrated on my Hierarchy of the Body card. The difference of the path toward death between the liver and the kidneys was the timeline toward death – the path was much faster when triggered by the kidneys.
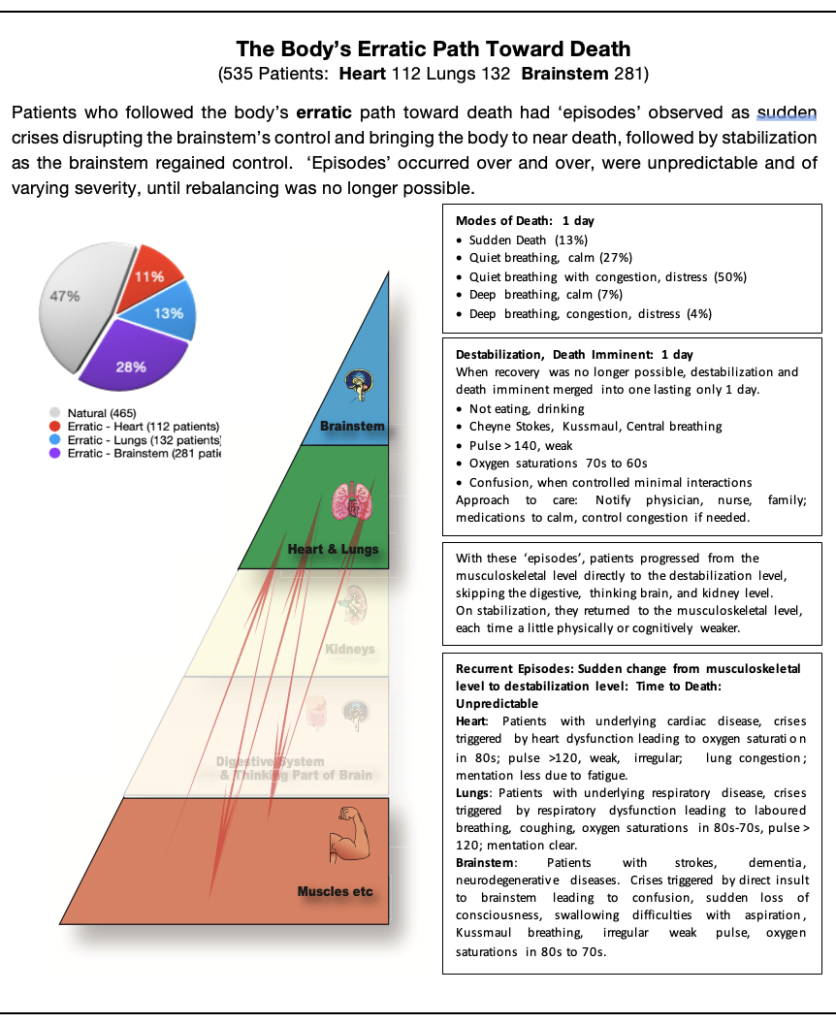
On review of the data, the patients whose life-threatening event was failure of the heart, lungs or brainstem had a very different path toward death. Caregivers observed ‘episodes’ at the musculoskeletal level indicating which essential organ was being attacked. Suddenly, patients deteriorated quickly from the musculoskeletal level to the essential organs of the heart, lungs, and brainstem, skipping the digestive system, thinking brain and kidney levels. The body was, suddenly, on the edge of death. With each ‘episode’ the patient’s death was indeed imminent for a short time. By the swift action of the brainstem, supported by medical interventions, the body stabilized and slowly recovered back to the musculoskeletal level, usually at a slightly diminished functional or cognitive level where no one could predict when another ‘episode’ would occur or how serious the next ‘episode’ would be. These episodes could occur sporadically over years. Or the next episode could cause enough damage to the targeted organ to cause rapid death. No one could predict. What was predictable – eventually, one of these ‘episodes’ would lead to rapid death. The word that best describes this progression to death for me is erratic.
The body’s erratic path toward death was so very difficult to predict:
If the organ affected was the heart, the ‘episodes’ were triggered by sudden heart dysfunction, leading to major fatigue even with minor activity, dizziness on standing, irregular and weak pulse over 120, congestion on breathing, oxygen saturation in the 80s, and diminished ability to think clearly and make difficult decisions.
If the organs affected were the lungs, the ‘episodes’ were triggered by respiratory crises, leading to observations of laboured breathing, coughing, oxygen saturations falling into the 80’s even with supplemental oxygen, and pulse rising to above 120. Mentation remained clear.
If the organ affected was the brainstem, the ‘episodes’ were triggered by a direct insult to the brainstem (e.g., bleeding or blood clot compressing the vessels to the brainstem), leading to a greater variety of symptoms including confusion, sudden loss of consciousness, weakness on one side of the body, swallowing issues with aspiration of food into the lungs, Central breathing, irregular or weak pulse, and oxygen saturations in the 80s.
Early in a patient’s journey, these paths toward death, often reversed with treatment, allowing the brainstem to rebalance the body’s functions. All observations seemingly returned to normal. But caregivers, who knew the patient best, knew that with each ‘episode’, their loved one did not completely recover to their former baseline activities.
The data reflects that when all the patients reached destabilization, meaning death was imminent, family observations indicated similar modes of death. The natural and all three erratic paths toward death merged into the same modes of death because the functions of the essential organs (i.e., heart, lungs, and brainstem) were so intimately integrated.
For the first time, I was able to validate my clinical experience, using our subjective and objective observations. Using my data as the foundation, I revised my former Hierarchy of the Body chart. The major differences are summarized below.
|
The Body’s Natural Path Toward Death (465 patients): Premonition signs of impending instability: 13 days Ø less eating; weight loss; slower thinking; and increasing fatigue. Destabilization signs: 6 days Ø no eating; no drinking; pulse >120; Kussmaul breathing; oxygen saturation in 70s; confusion, once controlled interactions were decreased. Death is Imminent signs: 1 day Ø pulse >140 weak; oxygen saturation in 70s to 60s or not measurable; confusion once controlled minimal interactions; observed Modes of Death; Gasping respirations. |
|
The Body’s Erratic Path Toward Death (525 patients, average onset to death) Recurring ‘episodes’ at the musculoskeletal level: Unpredictable Ø ‘Episodes’ differentiated the trigger: heart, lung, or brainstem failure Destabilization signs with Death is Imminent: 1 day Ø no eating; no drinking; Cheyne Stokes, Kussmaul or Central breathing; pulse >140, weak; oxygen saturation in 70s to 60s; confusion when controlled minimal interactions; observed Modes of Death; Gasping respirations. |
To present this information simply to patients, families and caregivers, I evolved my Hierarchy of the Body chart and created two separate charts:
Throughout the years providing care through my community practice my patients continually added to my knowledge of the ‘science’ and the ‘art’ of near-end-of-care.
As I reviewed the data provided through each of my patients’ journeys toward death, I discerned more completely the body’s adaptations to life-threatening assaults at near-end-of-life. Although my understanding of the body’s hierarchy of its essential organs was correct, the body’s primary path toward death, cumulatively for all patients, only followed the ‘natural’ path toward death in about 50% of the patients.
The other half of the patients followed the ‘erratic’ path toward death triggered by life-threatening assaults to the heart, lungs, and brainstem.
In patients with non-cancer diagnoses, most of the patients followed the ‘erratic’ path toward death, with destabilization leading to imminent death occurring very quickly when recovery from an ‘episode’ was no longer possible. Perhaps these factors contributed to the difficulty to judge the timing of a palliative care referral for these patients.
The data provided through my clinical records validated my Hierarchy of the Body chart when I presented the information in separate charts for the body’s ‘natural’ and the ‘erratic’ paths toward death.