
It must be clearly stated again – I did not believe my community palliative care practice would be sustainable. I was wrong! My patients and families were correct! They proved their ability to successfully stay in their own homes or a residential hospice until their deaths if they had a 24/7 link with a physician and community resources.
During the first six months initiating the network, I did see signs of success. There was a steady stream of appropriate referrals. I stabilized my new patients, provided symptom control, and most died quietly at home with their family. But it was a struggle. It felt like I was rushing from crisis to crisis. With the reluctance of families to talk with their loved ones about the reality of their situation early in the process, we often had those discussions during a crisis leading to much more stress for the patient and family and for me.
I realized I needed to allow the family to come to terms with their reality in their own time, but I was frustrated. Upon reflection, I decided to concentrate on areas of my practice over which I had control. I needed to improve the practical logistics ensuring that the crises were easier to handle. I spoke with several pharmacists in the community to explain my practice and that, frequently, I would need certain injectable medications urgently at near-end-of-life. They agreed to store small amounts of these medications for easy access when I needed them. I set up the trunk of my car with equipment to address the most common problems: for urinary retention, I now had kits to insert bladder catheters when needed at night; for wound care, I gathered dressing trays and materials to control bleeding; and when patients could no longer swallow and needed injectable medications, I had syringes and needles.
My goal was that if I could demonstrate to patients and families that crises could be quickly and effectively addressed, our relational trust would grow. They would be more likely to believe they could continue the care at home and begin to feel safe to discuss how to address future needs before the occurrence of significant crises.
Funding:
The Community Palliative Care Network was sustained for fourteen years with funding provided only by regular government billing and the use of the Palliative Home Care resources in the community available through new provincial initiatives.
Teaching:
To support the growing need for additional learning, I merely let it be known that I was available to participate in any community teaching sessions or discussions if requested. I used my digital summaries of the ‘science’ of palliative care to help in group presentations for nurses, personal care workers, etc. As the years went by, in preparing for these presentations, I rarely needed to change or update my slides for the ‘science’ of palliative care. However, through my experiences with patients in their homes, I constantly updated my presentations with what my patients and families taught me – their unique ‘art’ of near-end-of-life care.
Collaboration and Flexibility:
The community nurses were the first to notice I was taking a different approach. They believed in home care and advocated for their patients. If one of their patients did not ‘exactly’ meet the criteria for a referral, but the nurses believed they ‘were’ palliative, they would contact me and state, “Please visit this patient and family, you will understand the situation. We told the family you might not continue the care at this moment but even one visit would help us care for them better.” The nurses admitted to me a few years later, “We knew if we could convince you just to put one foot in the door, you would eventually agree to continue to care for these patients.” These incidents only reaffirmed that referral criteria should be flexible depending on the situation.
Throughout Canada, the recognition of the need for palliative care increased over the years. There was ongoing planning for different palliative care models in hospitals and communities in Ontario with some funding for clinical care delivery and teaching.
In 1999, the May Court Day Hospice opened, providing support to patients at near-end-of-life care through their day programs.
In 2001, the first Residential Hospice opened its doors in Ottawa. This provided an additional essential resource (9 beds) for patients who wished to remain at home but for physical or emotional reasons were no longer able to manage the care. Now they could be admitted to a community facility, set up specifically for near-end-of-life care, with their families close to them and with physicians who had provided care at home were seamlessly able to continue with the care.
Several nursing agencies with expertise in providing near-end-of-life care were set up in the community, adding to the government-funded nursing agencies for patients who wished to continue to stay at home until their death.
The Ottawa community of caregivers wanting to learn more about the provision of palliative care in patients’ homes set up teaching sessions and discussions.
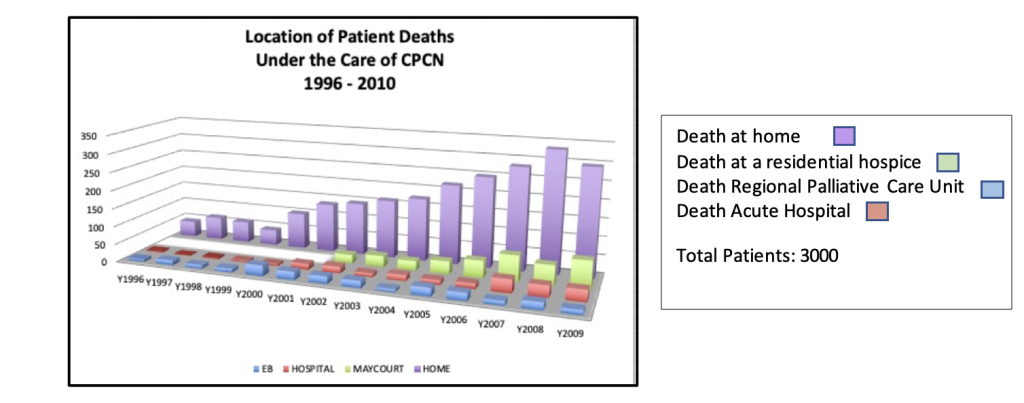
The graph below summarizes the Community Palliative Care Network’s expansion and successes in keeping patients at home or in a residential hospice from 1996 to the end of 2009. The practice was sustainable! The goal to provide care at home or in a residential hospice until death was achieved in over 80% of the patients.
Over the years, physicians joined the practice. After thirteen years, eight physicians, provided care through the Community Palliative Care Network and helped teach Family Medicine residents, through elective rotations, about palliative care and the power of the home visits. The personal well-being and safety criteria I had set for myself were met. I remained healthy and found balance with family members. I was never sued while providing palliative care in the community. When there were conflicting views, we found ways to resolve the issues. As well, I was not involved in any major car accidents, nor assaulted at night, and no one broke into my car looking for drugs. Patients and families were very supportive of my work, finding ways to provide me with safe parking.