
After I explained the body’s hierarchy for survival, in order for the patients and families to play a central part in the decision-making, they needed to understand what they were observing during their journey at near-end-of-life.
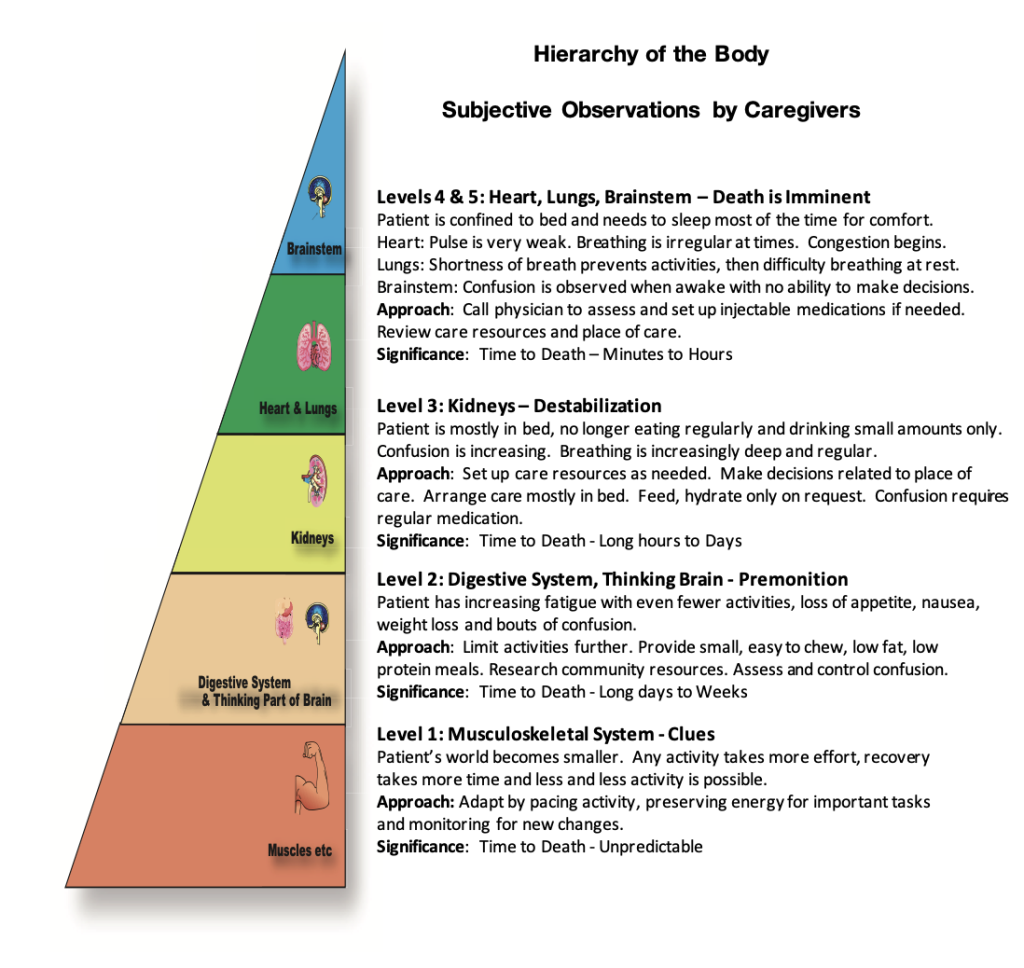
Together we reviewed the key subjective observations. Then, I explained the significance of each new finding and based on our new understanding the situation, we adapted our approach to the care.
Observable Evidence:
During my initial home visit, one of my first inquiries with patients and families was, “Please describe the patient’s level of activity: a year ago compared to six months ago, compared to during active treatment and after the last treatment. Please describe the level of activity at the present time.”
These simple inquiries allowed the families to review their history in a sequential manner and realize more clearly the changes in activity levels themselves. Caregivers recounted how many of the daily activities outside the home had diminished. They described that each activity took more effort and longer recovery time. We reviewed the patient’s essential activities of daily living, often realizing that stairs took more effort, and were attempted less frequently. Showering and personal care were less frequent.
At this level, I explained to families that there was no possibility of accurately predicting the timeline to death. But there were ‘clues’ demonstrating patients had less and less reserve energy to perform physical activities. The family often observed these clues and understood their significance first, knowing what activities were so very important to their loved ones that were no longer attempted.
Significance of the Clues:
The brainstem realizes that the body does not have enough energy to perform both non-essential activities and essential functions for survival. The brainstem, therefore, switches into its ‘survival mode’ taking the energy away from the muscles and forcing the patient to rest until all the high-priority functions are completed. Then, if there is any energy left, it gives a small reserve back to the muscles for its non-essential activities.
Approach to Care:
Many families observed their loved one’s world shrinking and thought, “They would be stronger if they exercised”, “They are just depressed”, or “If I plan more family activities, perhaps they would be happier and stronger.” Still, usually, the families had already changed their loved one’s activities out of necessity, planning fewer activities, and more rest periods.
I explained that the reality was NOT to plan more exercise and activities, but rather to monitor their loved ones closely, and preserve as much energy as possible while still allowing important activities to take place. I reinforced that by limiting activity they were already doing precisely what was needed. If their loved one used too much energy on non-essential activities, the brainstem would ‘push’ back, by initiating unpleasant symptoms to terminate the activity. The brainstem would NOT allow the body to be put at risk for a non-essential activity.
I then explained that the patient’s ‘world’ would continue to shrink. I suggested that together we needed to review all their loved one’s activities and decide which were the most important, finding ways to continue these activities by performing them in a manner to preserve as much energy as possible. Together, we reviewed the home environment to assess the barriers to essential daily activities as reserve energy continued to diminish. For example, “Would the stairs become a problem?” “Was there a plan for personal care when climbing the stairs became impossible?”
This was the first lesson at near-end-of-life. The brainstem is in charge of the body’s essential functions. The body has no choice but to follow its rules at each level of the body’s path toward death.
Observable Evidence:
The patient’s fatigue continued to increase; their activities continued to decrease. The patient’s appetite decreased variably, usually associated with fatigue after an activity, leading to weight loss. The patient slept longer at night, with increasing naps throughout the day. At times, there was mild confusion, usually associated with fatigue after a demanding activity. Clarity of thinking returned with rest.
Significance of Premonitions:
I explained to the families that they were observing ‘premonitions’ of the body transitioning to the level of the digestive system and the thinking brain. Again, these observed changes were controlled by the brainstem with the primary goal to preserve energy and use innovative measures to find new energy. When the brainstem has used all the reserve energy from the musculoskeletal system, it tries to find a little energy in the digestive system and the thinking brain. It starts by changing priorities for the digestive system by allowing the body to ingest just enough food for its day-to-day activities while stopping all storage functions, knowing the body has a reserve of energy in its fatty and muscular layers for emergencies.
When even digesting the small amounts of food essential for the body’s day-to-day needs takes too much energy, the brainstem, in its survival mode, starts to use the body’s stored energy for it essential needs. This leads to obvious signs of poor appetite and weight loss.
The brainstem also directs its attention to the thinking part of the brain. If the body is asleep, and performing fewer physical activities, there is less waste of energy. When patient becomes confused on and off, it is an outward sign of the brainstem and thinking part of the brain ‘clashing’. Eventually, the brainstem wins out and forces sleep. The thinking brain recovers through this sleep with a return of mental clarity. At this level of the body’s path toward death, we can make predictions of the timeline to death, not accurately, but in a range from long days to weeks.
Approach to Care:
The approach to care for the families was more difficult for them to understand. Often the families were most worried about the loss of appetite. They concluded that the patient’s fatigue and weakness must be caused by not enough nutrition. Therefore, they tried to entice their loved ones to eat more, tried to add high protein drinks and then asked their loved one to exercise a little to maintain their physical strength. Their hope with this approach was that their loved one would be more alert and able to do more activities.
I explained again that the ‘realistic’ approach to care was to monitor their loved one closely and to preserve as much energy as possible by allowing the body to determine how much sleep it needed and how much activity it could tolerate. The approach to nutrition was to carefully introduce meals after a period of rest, that were small, mainly low fat and low protein requiring the least energy to digest. Many patients had their favorite meals e.g., ice cream, various soups, etc. The families could offer these meals even if they appeared to be high in fats. Often, they were favourite foods because the patient had always been able to digest them easily. The families would quickly observe if they were tolerated. My key messages to families were that attempts to increase the amount of food ingested would NOT lead to more alertness and physical activity. The brainstem would simply get rid of excess food by causing nausea, vomiting or diarrhea leading to discomfort. The families would be the first ones to observe when their loved ones were approaching the next level of the body’s natural path toward death. They would witness more ominous premonitions of increasing weight loss, almost no eating, sleeping or in bed most of the time and no interest in social interactions.
Observable Evidence:
The families observed that their loved ones were almost always in bed. They often skipped meals, ate very small amounts, and drank only occasionally. They could no longer follow long conversations and were unable to make complex decisions, often demonstrating signs of confusion. The family would often be the first to observe that their loved one, during sleep, had short periods of deep, regular breathing with no apparent distress, clearing spontaneously.
Significance of the Destabilization:
I explained to families that their loved ones were on the edge of destabilization. The body had now transitioned to the level of the kidneys. The timeline to death was now more accurately predictable from long hours to days.
I explained to families that, again, these changes are controlled by the brainstem. The brainstem realizes the internal environment of the body is not being well controlled. For survival, the kidneys need to continue to efficiently balance the sodium, calcium, potassium, and acid/base balance in the body. When the kidneys start to fail, the imbalance becomes life threatening. The brainstem stops its quest to preserve energy. It starts to use all its energy to stabilize the kidneys’ function integrating with the heart and lungs. The brainstem will not allow any use of energy except for survival and therefore orders the body to sleep. If the families observe their loved one awake, calm, and asking for food or drink, it means internal balance has been achieved temporarily and the brainstem now releases a little energy to the digestive and thinking brain function. If the patient awakens confused, restless, and distressed, the brainstem is having difficulty restoring balance, and is struggling to make the patient to fall asleep.
Approach to Care:
Families urgently need to research community resources in preparation for future needs. They need to discuss and make decisions about the place of care in the near future when their loved one can no longer swallow medications and transfer out of bed. I reassure families that it is in the best interest of their loved one’s comfort to offer food and drink only when they are awake and requesting food and drink. If their loved one’s confusion is distressing, we need to discuss medications to help keep them calm and comfortable without overly sedating them.
Observable Evidence:
The patient is confined to bed, with the need to sleep most of the time for comfort:
If the heart fails first, families observe dizziness on standing or sitting, irregular breathing with congestion on and off.
If the lungs fail first, families observe shortness of breath preventing any activity increasing to shortness of breath at rest.
If the brainstem fails first, families observe confusion, distress when awake often combined with the above signs of lung and heart failure.
Significance: Death is Imminent
I explain to families that the heart, lungs and brainstem are integrated in their functions and dependent on each other. If the brainstem fails, there is no control over the functioning of the heart and lungs, so they quickly fail as well. If the heart fails, no blood goes to the brainstem and lungs, so they fail. If the lungs fail, no oxygen goes to the brainstem and heart, so they fail.
Approach to Care:
The key approach to care at this time is to know that this is about to happen and start planning before the crisis regarding the place of care, the availability of injectable medications, and 24-hour a day links with the community nurse and physician. As soon as the destabilization starts, these decisions must be implemented promptly. The goal of care at this point must emphasize comfort. The timeline to death is minutes to a few hours.
The caregiver who spends the most time with their loved ones, will observe both subtle changes and impending crises first
If they understand the significance of their observations, they will be able to direct the care of their loved ones, adapting to the changes early, to prevent crises while maintaining important daily activities.
When family understand the changes, they help direct the professional caregivers to control any crises promptly.