
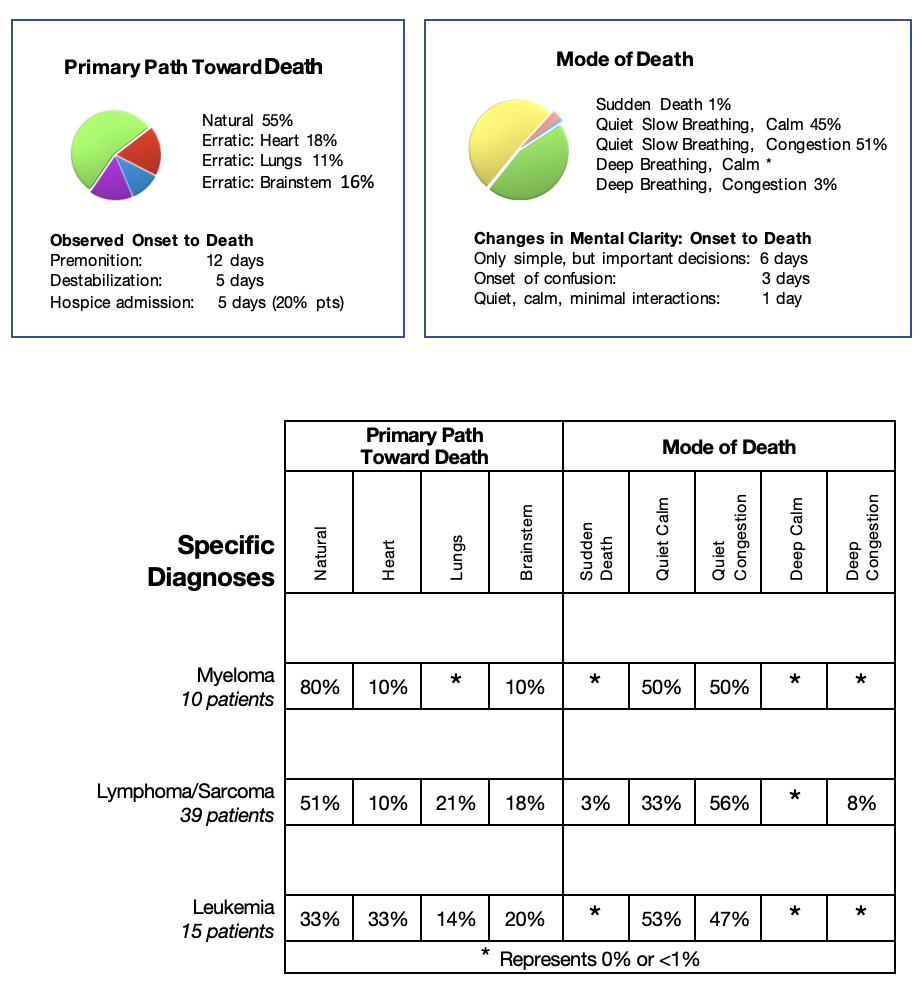
Although all the diseases in this category originated from blood-related cancers, the patients presented very differently in the early part of their illness, therefore, I decided to discuss each specific disease individually. At destabilization, these specific illnesses were very similar in their paths toward death.
Myeloma:
Patients with myeloma usually presented with increasing pain, mainly in the mid and lower back. Investigations revealed scattered bony lesions and bone marrow invasion.
Early symptoms were mainly related to bony pain. As the disease progressed, the spread was through blood vessels to the kidneys leading to the natural path toward death, throughout the bone marrow leading to the erratic path toward death triggered by anemia and heart failure, and into the brain’s covering tissue leading to the erratic path toward death triggered by brainstem failure.
Lymphoma/Sarcoma:
Patients with lymphoma/sarcoma cancers progressed through the lymphatic system, with deposits in any location in the body’s tissues containing lymph nodes. Initially, there were few symptoms. When the cancer started to spread locally the symptoms were not from erosion of the cancers, but from compression of organs, tissues, and blood vessels presenting as large masses attached to bones and muscles. When the cancer spread diffusely, patients presented with enlarged lymph nodes, and infiltration of the essential organs. If the spread was to the liver and kidneys, the patients followed the natural path toward death. If the spread was to the lungs, heart, and brainstem, the patients followed the erratic path toward death.
Leukemia:
Patients with leukemia presented with increasing fatigue, frequent infections, and episodes of bleeding. Investigations revealed anemia and bone marrow suppression.
As the leukemia progressed, the complications were different from other cancers. The patients were supported medically throughout most of their journey with blood transfusions to control anemia and antibiotics to treat infections. When these treatments were no longer effective, they quickly destabilized. If they suddenly developed an overwhelming infection, they followed the natural path toward death. If their anemia became life-threatening causing heart failure, or the cancer infiltrated their lungs or brainstem, they followed the erratic path toward death.
Specific Diagnosis: Sarcoma
Erratic Path Toward Death, Cardiac Trigger
Pre-referral Information:
When I met Alice, she was 16 years old, a beautiful, intelligent, outgoing girl, wise beyond her years. Her mother recalls that the whole room radiated with light when she was born. Her parents were unique in their work and philosophy of life. They had raised Alice and her sister with great love emphasizing independent thought, good eating habits with natural food, and a diverse education – everything to ensure that their children would grow up healthy and happy outside of the mainstream, including health care.
When Alice developed cancer, a sarcoma in the bone of her left upper arm, it was devastating news for the whole family, even more so for her parents, who truly believed their philosophy of life and health should have prevented any such occurrence. They were forced to turn to the mainstream health care system – and now that approach was also failing their child. Alice’s arm was treated with radiation and intensive chemotherapy. Although initially helpful, it became evident that the tumour was very aggressive, rapidly recurring, growing as a gigantic mass encasing her left upper arm, most of her shoulder and lateral chest. It was far too extensive to have benefited from surgery. Her parents were told as well that options for chemotherapy were almost exhausted. They were angry, afraid and did not know what to do, where to turn.
Initial Contact:
The team at the Children’s Hospital wanted to begin discussing near-end-of-life issues, but Alice’s parents were NOT ready. The team was unsure of Alice’s expectations and found it difficult to talk with Alice alone without her parents. They referred Alice to me for palliative care. I assumed I would build a relationship and prepare for care at home when treatment options were exhausted. But that was not the understanding of Alice and her parents, as became apparent within minutes of our first meeting. They accepted me to be involved but only to provide symptom control with visits to the home.
With that imperative, the conversation on the first visit could only be focused on Alice’s symptoms. She was up and about, still going to school. Her parents were now separated. Alice stayed one week at her mother’s home, the next week with her father. Alice and her parents denied pain from her tumour, stating that Alice just had occasional ‘discomfort’. She used Acetaminophen with Codeine on occasion with good effect. She was eating well, had no nausea, and her bowels worked well. She just wanted to have more energy to be with her friends and feel normal.
I could not delve deeper into my concerns even though I observed the urgency to have an in-depth discussion regarding the rapid progression of her illness despite her good functional ability. The tumour on her shoulder and chest was the size of a watermelon. I knew her deterioration was going to be very rapid and very soon. I wanted to prevent a major crisis and I needed to understand her worries, feelings and plans. I could not even try to address my concerns; it was not seen as my role.
My only option was to address Alice’s desire for ‘more energy.’ I suggested a trial of a medium dose of Decadron daily, observing the effect on her energy level, appetite, and her ability to enjoy life over a few weeks. If my intervention proved effective, perhaps Alice and her family would start trusting my expertise. The dose was strong enough to have an effect quickly, but then the amount would need to be rapidly tapered to a dose that would beneficial but cause no side effects. If the steroid was ineffective, it would indicate that Alice had little reserve energy, and I would have another marker that her progression would be very rapid. Perhaps we could start conversations about the future and her hopes and worries.
The trial was very effective quickly. Alice thought she was cured. Her parents were elated. Of course, because I was just the ‘symptom control’ physician and her symptoms were better, all felt my role was unnecessary. They ended my services before my next visit planned to reassess the situation and taper the dose. Inevitably Alice developed the typical long-term side effects of a steroid including swelling of her face, swelling of her ankles, trouble sleeping and mood swings. Alice and the family blamed the steroid, and of course, they were right! The dose was too strong. I immediately lost what little trust I had gained. The family stopped the steroid completely without tapering the dose, causing other uncomfortable symptoms. I was asked not to return to the home.
This scenario demonstrates the dangers of poor communication amongst the patient, family, and care team. In accepting the referral to care for Alice, I thought the family understood I was a palliative care physician. The pediatric care team thought if I was presented to Alice and her family as a palliative care physician, they would not accept seeing me. And that is exactly what happened anyway. If I had known the actual situation before the visit, I might have taken a different approach and been able to continue to provide support in Alice’s care or I might have refused to take the referral until my role was clarified.
On-going Care/ Observations:
Alice’s cancer progressed. Her parents continued to focus on new treatments that might prevent further growth. In consultation with the oncologists, Alice’s parents asked to have one more cycle of chemotherapy. The chemotherapy was partially effective but mainly problematic. The tumour did indeed shrink, but only the central area died, causing a central crater filled with dead and dying tissue, extending from the skin to the bone. Essentially, at least twenty pounds in weight, the tumour looked like a volcano. We could reach in and touch the bone of her arm about one foot beneath the tumour’s surface. The smell of the decaying tissue was overwhelming despite all attempts to dissipate the odour with scented candles and vapours. The oncologists clearly stated there could be no more chemotherapy.
Alice decided to stay at home until she died. Her parents agreed but they were overwhelmed. This tumour needed to be dressed twice each day. One experienced visiting nurse, trusted implicitly by Alice and her family, made daily visits to clean the wound and manage the dressing. Alice’s parents did the dressing themselves in the evening. This trusted nurse explained to Alice and her family that the care of her extensive ulcer was very complex. The only way the care could be achieved at home was to involve a physician with experience with this type of wound, who would visit frequently. The nurse knew me well and persuaded the family that I would be the only physician to achieve Alice’s request to stay at home comfortably until her death. Alice and her parents cautiously agreed, and the referral was made.
I met Alice at her mother’s home. Alice fully participated in the conversation though she was lying comfortably in bed. Her wound was extensively dressed and had been recently changed. It was not the right time to assess the tumour at this first visit.
Alice clearly stated, “I want you to help me die at home. My nurse says you are the only physician who will not be afraid of my wound so you will be able to help me stay at home. I trust her, I will accept your care now. But you must not prescribe a steroid. I do not have pain, just occasional discomfort, so you must not prescribe Morphine. I stay with my mother one week, my father the next, you will need to visit at both places.” Her mother was frightened but willing to fulfill her daughter’s wishes to remain at home.
This wound was nasty! I was now clearly seen as the “wound” physician. I knew the success of this wound care would be crucial to achieving Alice’s goal to stay at home. I would be visiting very frequently for these extensive dressings. I could assess my other concerns for Alice’s care in the background, quietly, over time. I did not need to worry about her pain for the present.
She had her acetaminophen with codeine and appeared very comfortable and cognitively very clear. If Alice had significant pain, she would demonstrate her discomfort during her efforts through the dressing procedure. The near-end-of-life issues would become very important, but if I controlled the wound, as Alice weakened, I would have opportunities to start these conversations. The place of care would need to be addressed later when Alice would not be strong enough to relocate each week. Even though Alice and her family had fired me in the past, I was confident in this family. The love displayed by her parents and extended family for Alice was so evident.
Fusion of the Science with the Art of Near-End-of-Life Care:
I knew I needed to focus on managing the care of this wound. I set up my next visit with the visit nurse and Alice to assess the tumour’s eroded area, the cleansing, and the dressing process. I had dealt with very extensive ulcerations in my career, but this was one of the worst and the most difficult to dress. Pieces of dead tissue fell off with each dressing change. Observing the process of cleansing, and bandaging, I confirmed that Alice appeared to experience little ‘discomfort’. However, I noticed the effort each wound dressing required of Alice. She always started the procedure by removing the old dressing herself, then soaking the tumour lying in her bathtub. She, then, walked to the bed, sat quietly, and steeled herself for the lengthy process. Alice, without the tumour, weighed about eighty pounds. She had to hold up this twenty pound tumour for over a half-hour. When it was finally over, she quickly and gratefully lay down to allow the tumour to be supported by her bed. I could see the effort in her face while sitting and how she quickly recovered when lying. I reflected to Alice that this procedure seemed to be tiring for her. She smiled and stated, “Not at all, I can do this.”
Alice observed my reactions to her tumour and its ulcerated area in that first visit. I passed the test – I did not appear to be frightened or ‘freaked out’ with the odour. She quietly permitted me to continue to be involved in her care. I knew the main issue to solve, if Alice was to remain at home was, “How could we change this dressing with Alice lying down, NOT needing to support the tumour as she became weaker or if her cancer became much heavier?”
Initially, I visited twice weekly with the nurse to assess the wound and determine the best dressing for now and discuss how to dress the wound with Alice lying down in the future. I soon realized just how much Alice loved her bath – she felt so light, so free, and there was no odour! As she weakened, she wanted to spend more and more time in the bath. The nurse and I decided to change the timing of the dressing, waiting for her parents to call as Alice finished her bath so she could bathe as long as she wished. This change pleased Alice – it made her feel important!
The nurse and I had one chance to make the dressing change easier for Alice, all done in the lying position. Alice was too weak now to adapt and agree to a procedure that was not obviously better for her. Our first attempt was not perfect. We prepared all the layers for the dressing while Alice was still in the bath so they could be applied at one time. We convinced Alice to lie to her right side to expose the necrotic tissue. As soon as she lay on her side, Alice found a balance point quickly, so that gravity held the tumour in that position without any effort from her. The dressing ordeal was so easy – the relief on her face said it all! The difference in comfort was so apparent to Alice that she agreed to continue to let us sort out the ‘bugs’ each day until we perfected the most efficient routine.
As the weeks passed, the wound care became more complicated, the erosions uglier and more extensive. The nurse and I decided that we, not the parents, should do the dressing in the evening. The relief her parents felt was evident. And Alice was a ‘picker’. The nurse was worried, reporting more bleeding from the wound some days because Alice would try to pick away at some dangling lumps. I addressed the issue by making another change to the timing of my visits. Her parents now contacted me about a half-hour before Alice finished her bath. With Alice’s permission, we had part of our visit while Alice was lying in the bath. She was relaxed and more open to discussing her daily activities and fears. I explained that I was a ‘picker’ too, and if she let me, I could pick away at the dangling lumps of the tumour while she was in the tub. I would stop if I saw blood in the water. She thought this was a ‘very cool’ idea – a good solution. For me, it was another successful step in solidifying her trust.
As Alice weakened, it became essential to make decisions about the place of care. Fortunately, the location of her care became obvious. Alice’s father had the best set up for the ‘bath’ – just off the main bedroom. So, without my input, it was decided that Alice would stay in her father’s home, and her parents would change their living arrangements each week.
At each visit, I would quietly assess the level of Alice’s pain. Alice continued to deny pain admitting only to ‘discomfort’ at times. Once, much later, she told me, confidentially, “You know, I do have pain at times.” I could see the effort it took to walk about, and I knew she was taking more acetaminophen with codeine. One day I brought up the subject of discomfort, first with Alice, then her parents. I knew that Morphine or Hydromorphone would be taboo, but I explained how we could use a pain patch, the smallest one, to replace or add to the acetaminophen with codeine for the discomfort.
I showed them a sample – a tiny plastic sticky patch to be placed on her good arm. I explained that it was not Morphine or a derivative of Morphine, but it was potent, it would cause less constipation than the codeine, and if she did not like the sensation or thought it was too strong, they could easily remove it. I clearly explained that though it was not Morphine, it was very powerful.
I observed the look on all their faces – they all wanted ‘something’ to better control Alice’s discomfort as she progressed. They examined the ‘small’ patch and felt it did not ‘look’ strong. And that was all I needed to convince them to try it. And yes, another success. Her parents saw Alice was more comfortable. They still worried that it might make her groggy, but they never rejected it. Now, Alice and her parents were self-directed. They did not use the pain patch in the usual way. Alice would remove the patch with her bath every day, maybe not put it on again or perhaps she would. I never knew exactly what she did with it, but I could see she was more comfortable. I was certain she would never use two patches and the ability to remove it gave her a sense of control. For me, I knew that I would be able to control Alice’s discomfort when she could no longer eat – another milestone in being able to keep Alice at home.
As I observed Alice weakening, I dared to briefly discuss some of the essential functions of life – urination and bowel movements. One day, I observed Alice climb the three stairs to her room. It was an ordeal, but Alice answered my inquisitive look, “I need to do exercise to get stronger!” After the dressing, I broached the topic. “Alice, when you progress further, this tumour will become so heavy that you may not have the strength to go to the bathroom to pass urine. You will need to learn to void lying down into a diaper. It is a natural process, and no one will mind.” As only a teenager can react, she chose to challenge me, “So how do I learn to do that. Will you show me when the time comes?” I answered, “Yes, if you want me to.” At the next visit she asked, “Will you help me pass urine in this diaper?” I sat beside her, and we used a ‘visualization’ technique. She succeeded to pass urine and have a bowel movement after which she smiled and asked, “I am finished now. Will you clean me up?” I smiled and, without hesitation, said, “Sure, tell me where the face cloths are.” She never asked me to perform these tasks again.
Alice reaffirmed what I already knew, which is easy to forget at times. If you tell a patient a significant truth for the future, remember that they are listening, and they will test you when the time arrives. If you are consistent, do what you agreed to do, you cement the trust in the relationship.
The Science of Blood Transfusions:
The benefits and dangers of transfusions depend on the timing of the transfusion in the progression of the disease. Alice’s parents could see that Alice was getting weaker. The nurse and I noticed that she was pale, and her tumour was softer, floppy, obviously bluish. Her parents asked the oncologist for a blood transfusion. Alice reluctantly agreed. When I arrived the following day to help with the dressing change, I first noticed that both her parents were in the room, backed against the wall, looking at Alice with fear in their eyes. I turned to Alice. She appeared comfortable, but I immediately observed why her parents were frightened. Her tumour had almost doubled in size, now tense, filled with fluid with large bulging blood vessels on the surface. Both parents looked at me and said, “No more transfusions!” Another obstacle I did not need to address.
With many of my patients, I discussed the importance of nutrition for the health of the body to build a reserve of energy to do more activity. I also addressed the futility of trying to nourish someone at near-end-of-life who is so close to dying that the body’s survival mode prevents food from being digested to preserve its limited energy for more essential functions. A blood transfusion provides nutrition to the body. When the body with cancer is given nutrition, the nutrients are spread throughout the body. That is good! But cancer does not follow the rules of the body’s survival. It captures most of the nutrients for itself and grows faster. This reality was so obvious when Alice was given the blood transfusion. The tumour voraciously took all the nutrients and fluid, appearing to double in size, while Alice’s body had no benefit. This was the objective evidence of what I had often told my patients when asked about feeding and blood transfusions, “Listen to your body. If you feel the benefit, you are doing what your body wishes – it is a good decision. If you feel no benefit or feel worse, stop! Your body is telling you it is the wrong approach to take.”
The Art of Addressing the Reality That Death is Approaching:
A few days later, during my regular visit with Alice during her bath she asked, “My girlfriend said she heard the adults talking. They said that I had just a few weeks to live. Now I cannot believe that. Look at me, my mind is clear, I have much to do, I am writing a book. There is no way that I will die soon. What do you think?” I had not been ‘cleared’ by her parents to talk about dying with Alice. Still, I gained Alice’s trust; I had to be honest with her. I stated, “I do not think they are far off.” She replied, “Oh my, you know I always thought I could beat this cancer; I did everything asked of me; I even talked to my tumour at night, you know, to convince it to stop growing. I always thought I could beat this.” Then she quickly changed the topic.
Premonition:
Alice was progressing more quickly now, and we observed several premonition moments, demonstrating how Alice would destabilize as death approached.
The first was a ‘near-death’ experience occurred during her bathing before the dressing change. Although Alice was weakening, her bath time was still very important to her. When she was in the bathtub, she was so happy and comfortable that she stayed longer and longer. But the trip to and from the tub was now very difficult. One Saturday morning, I found Alice in the bathtub as usual – but she was very different. She was very pale and could not speak. Her breathing was just shallow gasps. I told her to stay still, and not try to get up. I found her father in the other room. I told him not to ask any questions but to go to Alice, pick her up, put her on the bed and then stand back to let me control the situation. With Alice lying in bed on her back, I put on her supplemental oxygen. I told her to focus on my eyes, not move, not talk, but just look at me and breathe deeply. Both Alice and her father were shocked; they did not question and did precisely what I asked of them. Within five minutes, her breathing returned to normal, and her colour improved. I waited a little longer and then removed the oxygen. She called her father over and looked into his eyes, saying, “Promise me, dad, no more tests, no more transfusions, no more treatment, promise me, dad!” He agreed. The intensity of the moment was over. She smiled at her father and asked for bacon and eggs for breakfast. When I left the room with her father, I said, “Do you understand what happened?” He shook his head. I said quietly, “Alice almost died in the bathtub today.” He finally looked at me and said, “If that is how she will die, I will be able to handle it.”
This event was a strong premonition of what would happen to Alice as she destabilized. She would likely have heart failure caused by anemia, triggering an erratic path toward death occurring very quickly with minimal symptoms.
Continuing the Fusion of the Science with the Art of Near-end-of-Life Care:
Alice had ‘learned’ and now ‘believed’ her reality. That belief was evident the following morning when Alice did not ask to have a bath and during her dressing change, she stated, “So ok; I know I will die soon. Remember I must die at home. Now I have three requests for you: Visit me daily, but do not hover; I have things to do. Remember – no Morphine. And I want you to tell me about 15 minutes before I die. I will have things to say to my parents and family.”
Alice’s third request was so tricky. I had to respond to that request truthfully without just dismissing her. I stated, “None of us are very good at predicting accurately when someone will die, but I am very good at predicting when you are not going to die
So, after I do the dressing every evening, by checking your tolerance of the process, your pulse and oxygen saturation, I will tell you if you are not going to die overnight.” That was acceptable to her.
I also took the opportunity to ask her. “Alice, what frightens you the most?” She quickly answered, “I am afraid that no one will remember me.” After thinking a few moments, I asked, “Alice, I do not think there is any danger that your family will ever forget you, but I wonder if you can do me a favour for my patients. Would you let me tell your story, to tell others all the things you have taught me so that I can help many other people going through the same journey – that way, you will never be forgotten.” Her eyes shone, she smiled and said, “Oh yes!”
Alice did indeed have things to do. And one week before her death, she was still planning. I did not hover, and I did not give her Morphine. I visited every evening to do her dressing and faithfully told her as I left that she would not likely die overnight. One evening I decided as a trial not to do so. “Was making the prediction each night really of value to her?” As I walked to my car, I heard her uncle running after me. I turned, and he asked, “Alice said you forgot to tell her if she was going to live through the night and told me to run after you, to find out.” I guess I had my answer.
Destabilization:
A few days before her death, Alice planned her birthday party. She invited her family and all her caregivers. She told us to dress up. With her family, she organized the balloons and the refreshments. We all arrived, but she was too tired to join us (as we had expected). However, it was fortunate that both the nurse and I were present because Alice had a significant bleed from her tumour during our visit. The nurse and I were able to quietly change the dressing and add a pressure pack into the depth of the tumour to control the bleeding without anyone, even Alice, aware of this life-threatening event. This was the destabilization event. We slowed the bleeding but could not stop it completely. We knew it would continue to ooze relentlessly until she died. Indeed, she would follow the erratic path toward death triggered by heart failure.
The next evening, Alice was very weak, barely able to speak. It was the first night both of her parents had planned to stay over together. After the dressing, as I was leaving, I explained to her, as promised, that she might die through the night. A tiny, weak voice asked, “I don’t know how to die, please, tell me what to do.” I reassured her that she was doing exactly the right things. Although I thought she was too weak to understand, I explained the process quietly while sitting beside her.
“Tonight, your body is telling you that you are exhausted and need to rest – you are doing that. Follow your body signals. If you are thirsty, ask for a drink. If you do not feel thirsty, do not drink, just rest. Let your family care for you. It is alright to let go and follow what is waiting for you.” To my surprise, a tiny voice answered, “I will try.
I then spoke to both her parents separately. I indicated that Alice had a good chance to die overnight; her pulse was feeble, her oxygen saturation was about 70%. I explained the ways of dying. Two ways would result in sudden death with either her heart stopping or no oxygen going to her brain – there would be no discomfort. The other ways would be the result of her lungs or heart running out of energy. If her lungs failed first, she would drift into sleep and die quietly. If her heart failed first, she could be distressed with congestion and a sensation of drowning. I stated that I could inject a medication, Scopolamine, to dry secretions and make her sleepy and relaxed, letting her die in any of the ways in her sleep. As I expected, both parents, separately, refused the injection.
I then advised her parents that I lived about a half-hour away. If Alice did become distressed, it would take time for me to visit and another half hour for the medication to work. Both again refused; they would stay awake with Alice and comfort her.
In the middle of the night, Alice’s father called me. He was distraught, observing signs that Alice was distressed and felt guilty because he had refused the medication. When I arrived, within a half-hour, Alice was lying on her favourite mattress on the floor with her mother and father beside her, her sister sleeping on the bed close to her, and her beloved dog kept watch just beside her. Now she had summoned her physician, who had promised she could die at home. Her breathing was not laboured, not congested. We observed simply tiny gasping breaths, strong evidence that her death was imminent. I reassured her parents that they had made the right decision about the medication. Alice had no need for medications. She just needed her family close to her. She died quietly a few minutes later.
The beginning of my doctor-patient relationship with Alice and her parents did not go well. I was asked to visit Alice under false pretexts, and Alice and her family did not have a clear understanding of my role. It did not end well. I was told not to return to the home, so I had no possibility of participating in Alice’s care. When their most trusted nurse convinced Alice, and her parents that I would be the only physician able to care for Alice’s wound at home, and the nurse convinced me to try to help one more time, I made sure that I followed the rules outlined for me by Alice and her parents. By managing her wound care, we built trust in each other, and Alice fulfilled her wish to stay at home.
I learned so much from Alice throughout her journey as I explained throughout the description of her story. The most important lesson was about trust. Alice started to trust me when she believed that with my help, she could stay at home. I demonstrated to her that I had the knowledge to deal with her complicated wound – I knew the science. Once we started building trust, she began to confide in me. She helped me learn the art of taking care of her. And beyond that, as caregivers, she reminded me that the more you are ‘trusted’ by a patient, the ‘greater’ the responsibility to respect that trust. I promised Alice I would share her story to help others and demonstrate how vital her journey would be to help others. I hope this summary of her journey honours the trust she gave me.
My relationship with Alice’s parents was essential to caring for Alice at home until her death. We rarely talked. Alice accepted me, and they wanted to do all they could to make Alice happy, so they tolerated me. Alice’s father considered me “Doctor Death.” I knew that they were overwhelmed with Alice’s illness, wanted so much for Alice to live and tried to do everything possible to make her happy and enjoy what life she had. They never interfered with my care for Alice. I tried not to challenge them unnecessarily.
I was surprised when Alice’s mother invited me to Alice’s funeral. Her mother invited all her caregivers, including myself, to this very personal funeral held at their home. Even more surprising was a call by Alice’s father a few months later. He explained that he had been so emotionally overwhelmed with Alice’s illness that the whole process was a blur. He was trying to deal with his child’s death, but he could not remember what happened in those last few months. He asked if I could please meet with him and go through each step of her journey. I was pleased to do so.