
When I gave presentations to professional and family caregivers, I usually used my Hierarchy of the Body card to explain the body’s path toward death and the significance of each of the signs throughout the journey. My audience listened carefully and understood at a ‘thinking’ level. However, when I illustrated the science with real-life experiences, they started to understand with their ‘heart’. Each person looked back at personal experiences and made connections with personal journeys They started to understand how patients and families could add their own unique art to their journey.
In Section D, I explained the unchangeable science of the body’s journey at near-end-of-life and for the first time I was able to verify these explanations with the evidence given to me through my experience with 990 patients. This section interprets and synthesizes the full data set to illustrate the paths toward death. By linking my patients’ gifts through their shared journeys, the data comes alive to support future patients and families. These journeys continue to respond to the initial questions asked by my patients and families, “How long?” and “What will the journey be like?” Now, it adds a more explicit response to, “What will the journey be like, specifically, for us?”
The unique patient journey within each group is shared in this journal with the permission of each patient while I was caring for them. After I wrote the summary of the journey following their death, I contacted each family, asking them to read the story to make sure I had captured the essence of the journey, and to ask permission again to share the description in my journal. Names were changed to ensure anonymity when requested by families. Each journey shares real near-end-of-life information of patients diagnosed with a specific disease. The narratives highlight the importance for patients and families to understand the science in order to fully participate in the decision making adding their unique art to enhance their own lives as they approach death.
As I stated previously patients were referred to me for near-end-of-life care irrespective of their diagnoses. Of the 990 patients in my study group, patients challenged me with over fifty diagnoses. To present this data, I divided patients into cancer and non-cancer categories. Then, I subdivided each category into five groups by similar primary sites of progression toward death. The following pie graphs summarize this information.
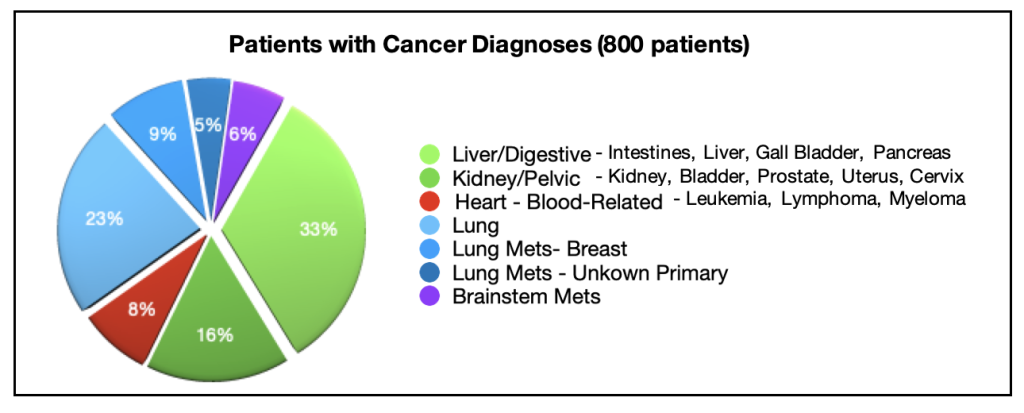
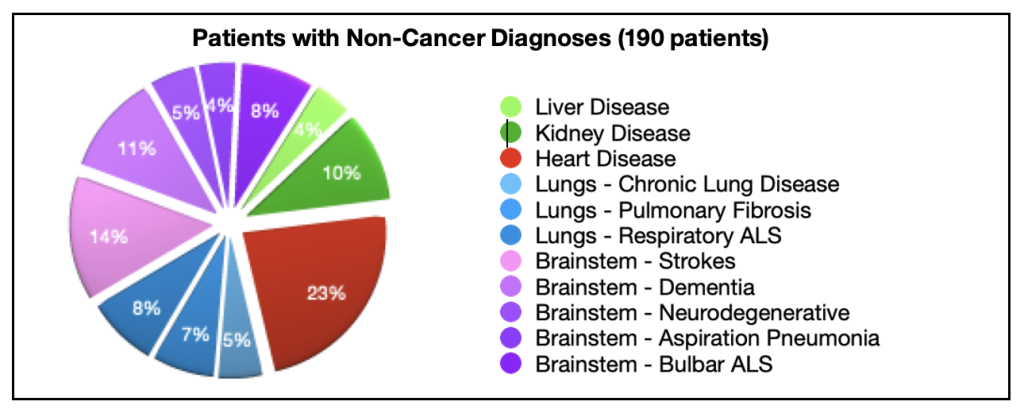
Knowing that readers may often be interested in a specific disease, this section of my journal, relates to each of these groups, divided into separate chapters for easy reference. Note: It is important to have read earlier chapters to understand emerging terminology (e.g., natural and erratic paths toward death and modes of death) before focusing on one specific diagnosis.
Chapter 26: Overview of Patients with Gastrointestinal Cancers:
Esophagus, Stomach, Intestines, Liver, Cholangiocarcinoma, Pancreatic
Chapter 27: Overview of Patients with Kidney/Pelvic Cancers:
Ovaries, Vulva, Uterus, Cervix, Kidney, Bladder, Prostate
Chapter 28: Overview of Patients with Lung, Breast, Unknown Primary Cancers
Chapter 29: Overview of Patients with Blood Related Cancers:
Myeloma, Lymphoma/Sarcoma, Leukemia
Chapter 30: Overview of Patients with Head and Neck, Brain Cancers, Melanoma
Chapter 31: Overview of Patients with Non-Cancer Liver Disease
Chapter 32: Overview of Patients with Non-Cancer Kidney Disease
Chapter 33: Overview of Patients with Non-Cancer Heart Disease
Chapter 34: Overview of Patients with Non-Cancer Lung Disease
Chronic Lung Disease, Pulmonary Fibrosis, Respiratory ALS
Chapter 35: Overview of Patients with Non-Cancer Brainstem Disease
CVA, Dementia, Parkinson’s, Aspiration Pneumonia, Bulbar ALS
Each chapter in Part E features:
The schematic below provides an overview of the information compiled for each group of patients. Analyzing this data responds directly to three questions, “How long do I have to live?”, “What will the process of dying be like?” and “What will the journey be like, specifically, for us?”.
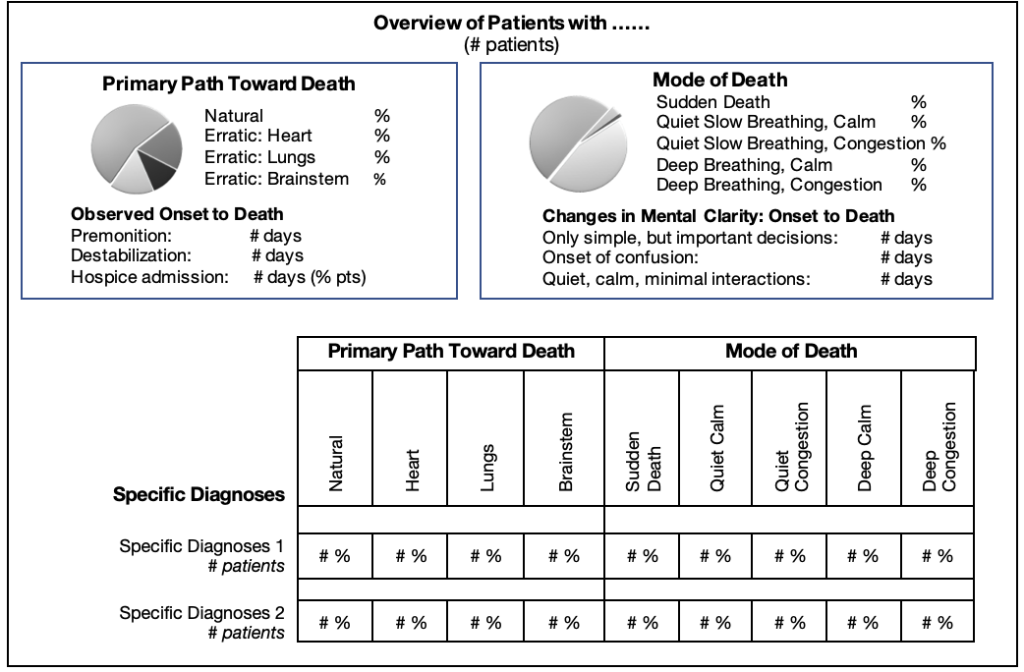
I encourage you to pinpoint the science of the body’s shutting down process while identifying the art of care responding to the uniqueness of each patient and situation.
Reading patient journeys may evoke strong emotional memories of a loved one or a friend. It is natural to make your own personal connections. I admit that reading my family’s journeys still brings tears to my eyes.
While Reading:
Take the time to pause and reflect.
Reach out to share your feelings and memories with family or a trusted friend.
Consider discussing how these journeys resonated with you, affirming or challenging your thinking.