
Probably the most frightening aspect of near-end-of-life care for patients and families is the development of distressing symptoms that are perceived to be difficult to control without adversely affecting the patient’s quality of life and decision making ability.
After patients had been told by their specialists that they would no longer benefit from active treatment, they were told that a referral had been made to palliative care for ongoing symptom control. Patients and families referred to my community palliative care practice were often very apprehensive, emotionally overwhelmed with many questions and fears. They had been given terrible news about their illness. They had lost their known links to the cancer clinic. Now, they had to develop a doctor-patient relationship with a new physician without knowing any details of the care awaiting them.
Some patients were very vocal, explaining their wishes as soon as I asked them to tell me about their journey from their diagnosis to the present. As they finished the description of the journey, they summarized their feelings by clearly stating:
“I know the specialists told me I was dying, but I do not feel like I am dying. I am going to keep fighting!”
“Do not interfere with the medications that have helped me so much over the years. I do not wish to hasten my death by stopping these essential medications.”
“I wish to be comfortable. I will take some new medications for my symptoms, but my mind must remain clear to enjoy the time I have left with my loved ones.”
Their families often admitted their fears as well:
“I am afraid that new and strong medications will make my loved one too sleepy or, worse, hasten their death.”
“I am afraid of needles. How could I possibly give injections?”
Over the years, experience taught me that these questions were in the minds of all my patients and families even if they did not express them verbally to me.
I also knew, from many conversations, there was tension between my hospital colleagues and the community palliative care physicians. Many hospital physicians felt care at home involved simply ‘holding a patient’s hand’ and giving medications that would keep a patient calm and comfortable but often cause drowsiness.
Therefore, when my brother and I created the digitalized patient database for my near-end-of-life community practice, we imbedded a section into the visit notes devoted to the medications I prescribed where I recorded: the start and stop date of the medication, the name, dose, frequency, and method of delivery. In my assessment notes, I recorded the symptoms triggering the need for the medication, the patient’s mental clarity before and after the medication was started, and its benefits and side effects.
During my extensive review to validate the data of each patient’s path toward death, I extended my review to encompass my approach to symptom control. I wanted to verify if I had been able to dissipate my patients’ and families’ fears by achieving good symptom control up to their death without adversely affecting patients’ mental clarity.
My initial goal for symptom control was to optimize the patient’s present medication regime without making any major changes. I involved my patients and families in the decisions from the first visit. I tried to create opportunities to optimize their medications to precisely meet their unique changing needs and to demonstrate that I had listened to and understood their challenges. I explained that I would be taking a regular ‘family physician’ approach to symptom control, concentrating on the ‘benefits’ rather than worrying too much about the ‘long-term side effects’ of the medications.
Together, we reviewed the medication regime already in place and responded by:
I reviewed patient’s present symptoms and asked permission to try small doses of new medications in the future in line with their goals. However, if the patient’s symptoms were controlled, I did not make any additions to their regime during the first few visits.
Specifically, if pain was present in the early course of the patients disease, it remained a symptom needing control. Generally, the intensity of pain did not increase toward death, mainly because it was no longer exacerbated by activity, eating or drinking. The major change in the pain regime was switching to an injectable form of the same medication as the patients weakened and were no longer able to swallow.
When the patients, families, nurses, and I started to observe premonition signs demonstrating progression toward death, it was time for me to act. I approached symptom control with three goals in mind. First, I needed to quickly stabilize any crisis to achieve comfort for the patients and to solidify their trust in my clinical skills. I always started with the medications familiar to the patients with small increases in the dose, or frequency, or a change in how the medication was administered.
Second, once the crisis was controlled, I asked the patients and families if we could discuss possible future or more serious crises. We reviewed the ‘trigger’ factors for the crises in the past. Then we tried to find ways to prevent these crises by achieving the goals of an activity with less expenditure of energy and by resting before, during or immediately after the activity. Third, I used the opportunity to review the body’s path toward death and discuss other crises likely to occur in the future, explaining the symptoms, the medications that could be used to control them and the routes of administration available.
When I observed my patients following the natural path toward death, I knew the crises would be less distressing and more predictable, so there would be time to review the issues whenever they occurred and sequentially make plans. When I observed my patients following the erratic path toward death, I knew the crises would occur suddenly, be more serious, more difficult to control and often life-threatening. Usually, I could control the first few crises using an approach effective in the past. Still, I took the opportunity to explain to patients and families that these crises would continue to recur suddenly and with increasing severity.
We needed to develop new strategies including the use of injectable medications before crises occurred to control them quickly and efficiently. If the patients and families were open to these discussions, I asked permission to order equipment and a few vials of injectable medications to bring into their home for future needs. Occasionally to help control a moderate crisis, I asked the patient and family if I could try a new medication, administered orally or by injection, as a trial, to control the symptoms without adversely affecting the patient.
Destabilization: Merging of the Paths with Death Imminent
I explained to all my patients and families that when patients destabilized, meaning the liver, kidneys, heart, lungs, and/or brainstem were under attack, no matter which path, toward death they were following, (i.e., natural or erratic), the paths merged.
The three most essential organs for life, heart, lungs, and brainstem, were intimately interconnected with each organ dependent on the others for the survival of the body. Their failure always led to the same constellation of symptoms. When the natural and erratic paths toward death merged at destabilization:
Lung failure caused shortness of breath, laboured breathing, distress at rest.
Heart failure caused dizziness, weakness, congestion at rest.
Brainstem failure caused severe confusion, restlessness, seizures, nausea.
The medications to control them were very similar.
Patients following the natural path toward death tended to destabilize with the failure of one essential organ first, either the heart, lungs, or brainstem, followed by a predictable domino effect on the other two essential organs hours to a few days later. In my review, the timeline from destabilization to death was 2 to 4 days.
Patients following the erratic path toward death, no matter which essential organ triggered the failure, the other two interconnected organs failed very quickly. The timeline from destabilization to death was often only 1 day.
Medications for Symptom Control
In analyzing the patient data at destabilization, I discovered that I used only ‘five’ medications on a regular basis to effectively control all the symptoms:
See the chart on the following page illustrating a summary of the medications I prescribed for these symptoms.
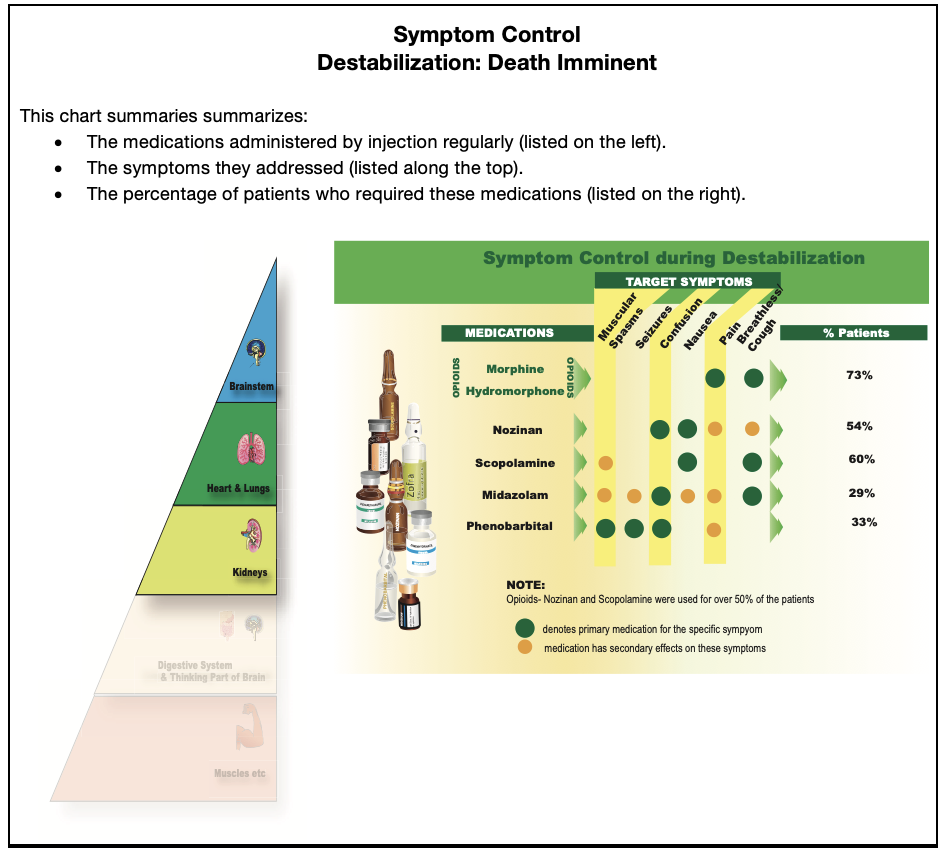
The data from my patient notes demonstrate two key facts:
Regular, injectable medications were required for over 50% of the patients.
Regular, injectable medications were only started a few days before death.
For the families, the beginning of destabilization was a key event in the care of their loved ones. I knew they were emotionally overwhelmed. I had experienced these emotions personally in the past. I knew they were afraid of doing something wrong that would lead to devastating consequences for their loved ones.
The families and I had spoken as the premonitions had become more ominous, about the need for several injectable medications to control the symptoms that could arise in the future, but those had been theoretical discussions. At the beginning of destabilization, impending death of their loved one became real. The need to start injectable medications was obvious to the family when their loved one could no longer swallow. Decisions to continue the care at home had to be made immediately. I needed to know if the family wished to accept the responsibility of care at home until death and could they manage the practical journey of care at home until death, most likely requiring the administration of injectable medications.
After the initial crisis at destabilization was controlled, I always took time to explain to families exactly what they would observe and what they would be expected to do if they decided to continue the care at home. First, to help alleviate their fears, I explained what they would NOT need to do regarding the medications. The nurses or I would visit daily. We would prepare the exact dose of the medications, set up a system for injection that would not require a ‘needle’ or an injection into the skin, and teach the family the administration technique. The nurses and I would take the responsibility to administer the medications as often as possible during our daily or twice daily visits.
Second, I explained what they WOULD observe about the medications:
Third, I explained that I would allow families to ‘hold’ a dose of medication if their loved one appeared very comfortable, and they were fearful of giving too much medication. Still, I reminded them that it would take at least 30 minutes to regain control of the symptoms if they let the medication wear off.
Fourth, I explained I would NOT allow families to give medications more often than I had prescribed. If they felt their loved one was uncomfortable, they were asked to call me to discuss their concerns and together we would decide what to do. I would always take the responsibility of the final decision about the administration of any medication.
After these explanations, I asked the patients and families to decide if they wish to continue the care at home, to transfer their loved one to a residential.
At the hospice the nursing staff would take over the responsibility for the clinical care, while the family could stay at the hospice to support their loved one.
The data demonstrated:
For the patients and families who opted to stay at home, I spent more time to discuss two additional medications, not used as often, but at times very valuable additions to better control the symptoms.
Phenobarbital, with a duration of action of 12-hours, was rarely needed in patients following the natural path toward death but at times could be valuable for restlessness at night, allowing both patient and family to have quiet nights. It was needed for most of the patients following the erratic path toward death, triggered by brainstem failure, especially for seizure and confusion control. I explained that it was administered by the nurses, NOT by the families, usually started at bedtime to prevent drowsiness in the day, but if seizures were not controlled, it would be given twice daily.
Midazolam, with a duration of action of 1-hour, was administered in the same manner as Morphine, Nozinan and Scopolamine. It was useful to help ‘top up’ control of confusion, muscular stiffness, and shortness of breath when the regular medication did not last the full four hours. It was often started early for patients following the erratic path toward death triggered by lung ‘episodes’, to help them recover quickly from respiratory distress after activity, while minimizing ‘hangover’ drowsiness.
Cognitive Clarity
When, I started to introduce new medications, I was very aware of my patients’ goals of comfort with a clear mind to enjoy time with family. Often patients and families refused medications that I knew would be effective and needed on a regular basis because of the fear of drowsiness and impaired ability to make decisions. They needed to be reassured frequently. They often accepted the medication for a few doses, then stopped the medication to test for themselves its effectiveness for their symptoms and the negative effects on their mental clarity.
General Verification from the Data:
Patients Following the Natural Path Toward Death:
Patients Following the Erratic Path Toward Death:
Changing Goals of Care at Destabilization:
For all the families, when death was imminent, I had discussions about their goals for symptom control under the new conditions. Although the initial priority was mental clarity, most families observed that whenever their loved one was awake at this stage, they were confused and distressed. Families’ goals changed, expressing the desire for their loved one to have comfort first rather than mental clarity as they approached death. Based on this shift in goals, together we set up a medication regime to ensure their loved one was comfortable above all, though we still tried to find ways to achieve some periods of lucidity with meaningful interactions of the family with their loved one.
Symptom control leading to comfort, while maintaining clarity of thought, was a high priority for the patients and their families.
Families were often frightened with the rapid changes at destabilization, with their loved one no longer able to swallow and the sudden onset of a myriad of symptoms. When the nurses and I explained the medications, their administration, and provided a 24/7 link with the family to support them, 75% families decided to continue the care of their loved one at home until their death.
As verified by my clinical data, over 50% of the patients required regular injectable medication for symptom control from destabilization to death. I used only ‘five’ medication groups for symptom control, and these medications were required only within the last few days.
Most patients died quietly, comfortably with family at the bedside or nearby. We were able to maintain the patient’s clarity of thought until the last few days when it was the body, itself, that lost control of cognitive thinking, not the addition of medications for symptom control.