
To play an integral role in decision-making for their loved one, families needed to be introduced to and understand the significance of another set of observations – the key objective signs I assessed during my visits.
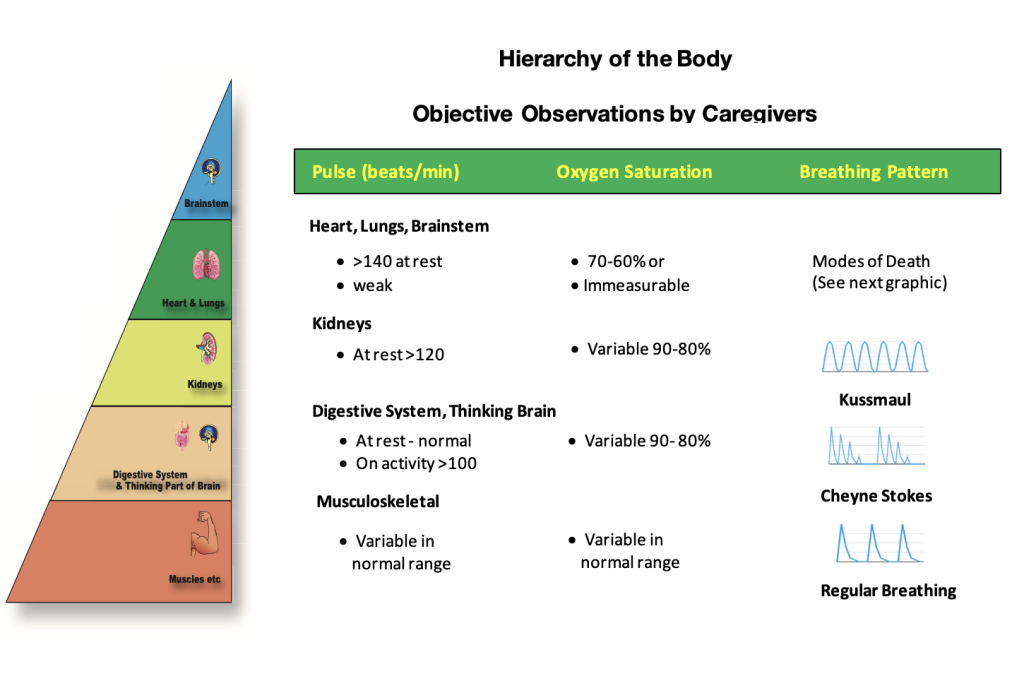
When families understood the objective findings of pulse, oxygen saturation and breathing patterns, at each visit, they could fully participate in the discussions reviewing the evidence and adapting our approach to the care of their loved one.
Pulse and Oxygen Saturations:
When I first started my community practice, at every visit, I measured my patient’s pulse and quietly observed their breathing patterns. When, a few years later, I had access to a small, portable pulse oximeter, I started to use this instrument to measure my patient’s pulse and oxygen saturation. I found it extremely helpful in evaluating the patient’s symptoms to give the family advice on the activities that could be safely performed. I used the results to plan the timing of my visits to anticipate and control crises quickly. I knew this information, coupled with an understanding of the significance, would also be very valuable to help families in the care of their loved ones. When the pulse oximeter became available at a very reasonable cost, I offered the instrument to each family. Most were pleased to have this extra tool. They could now measure their loved one’s pulse and oxygen saturation between my visits.
Breathing Patterns:
Another very valuable set of objective observations were the variations in breathing patterns. Families often observed these variations before the visiting nurses or physicians. I needed to explain the different breathing patterns and the significance of each variation.
At the musculoskeletal level of the body’s natural path toward death, there was little need for these objective measurements and observations on a day-to-day basis. Still, it was a good learning experience and provided objective markers for the family to use when their loved one’s world was shrinking with activity requiring more effort. Families, by experimenting with the oximeter, learned for themselves the oximeter’s usefulness and its logistics. For example, when the family noticed their loved one became more breathless with climbing stairs, I suggested measuring the pulse and oxygen saturation before and immediately after the activity. If the pulse and oxygen saturation remained in the normal range (i.e., pulse <100, oxygen saturation >90%), patients simply continued the same activities without worrying. If the pulse rose above 100, with normal oxygen saturation, these measurements, though not life-threatening, gave the family a level of confidence to continue the activity with adaptations to preserve energy.
At the musculoskeletal level, the breathing patterns were those well known to the family. Some patients snored deeply at night, and some had sleep apnea using a breathing machine to help regulate their breathing during the night. Most patients just had very regular breathing with a quick inspiration and a long, slow expiration. If patients had slight variations in this pattern and demonstrated these variations over the years without progression, they were of minor significance in the body’s natural path toward death.
As the body’s shutting down process reached the digestive system level, the family observed their loved one’s physical activity continued to take more effort. At rest, there were still no changes in breathing, pulse, or oxygen saturation. The family usually had gained some experience in using the oximeter and would report to me that it took less and less activity to cause the pulse to rise, at times to 120 with the oxygen saturation lowering to the high 80s. They described how they had already made changes in their approach to care by planning a rest period or cancelling an activity until all the numbers returned to normal.
I explained to each family that these changes were not life-threatening, but signs that the body had less reserve energy and any activity more quickly stressed the essential functions of the heart and lungs. Still, I took the opportunity to explain that in near the future, as the body relentlessly lost more of its reserve energy, they may be the first to notice a very frightening change in their loved one’s breathing pattern, initiated by the brainstem, to try to preserve a little more energy.
The brainstem, ever vigilant is always trying to find new ways to preserve a little extra energy for its vital functions. The regular breathing pattern produces an oxygen reserve available in case of emergencies. We know this fact because we can hold our breaths for varying lengths of time without danger to ourselves. At night, when the body is asleep, the brainstem knows there is no need to maintain such a high level of reserve oxygen and sends an order to the lungs to stop breathing for seconds to a minute. The oxygen level remains within acceptable levels during that non-breathing phase, but quickly the carbon dioxide in the blood elevates. (Unfortunately, we cannot measure the level of carbon dioxide in the body easily in the home). When the carbon dioxide elevates beyond a safe level, the brainstem sends another message to the lungs to restart breathing to clear the carbon dioxide through its expiratory phase.
The family observes a recurring pattern: a period of no breathing, followed by several deep breaths, slowly decreasing in amplitude, and then stopping again.
Usually, their loved one remains asleep, not distressed. Occasionally, on reinitiating the breathing, there is a startle reaction stimulating them to awaken for a few minutes.
The longer the ‘non-breathing’ period the more frightening this breathing pattern is for the family. When I demonstrate to the family that through this cycle the pulse remains in the normal range and the oxygen saturation actually rises in the non-breathing phase, they are a little reassured, but only a little. This breathing pattern is common but does not occur in all patients. It is called Cheyne Stoke respirations after the names of two physicians who initially described and reported the pattern to their colleagues.
The Cheyne Stokes breathing pattern does not signify a life-threatening event. It usually occurs just before the body transitions from the digestive system level to the kidney level. The breathing pattern does become a more ominous sign when it presents more frequently with lengthening non-breathing periods, and oxygen saturations lower into the 80s during the breathing phase. At that point, it is a premonition that warns, “Pay attention, destabilization will start soon.” If we think about it intuitively, the fact that the brainstem now orders the lungs to stop breathing to save a little energy, would seem to signify that there is very little reserve energy available for the body’s survival. The timeline to death is days to a few weeks.
Families have difficulty discerning the body’s transition to the kidney level. The subjective observations are much the same as at the digestive and thinking brain level, only more severe, but there is variability from day-to-day. However, there is one clearly ominous objective sign. The family observes deep, regular breathing, with forceful inspiration and expiration. Usually, their loved one is asleep, not distressed but appears to be working very hard – and they are!
This deep regular breathing pattern is called Kussmaul breathing. It is initiated by the brainstem when a patient’s kidneys are failing, no longer able to clear excess acid from the body. During forceful expiration, carbon dioxide combined with water is forced out lowering the acid in the body. It is meant to be a temporary, emergency measure because it is highly energy-depleting. It signifies that the brainstem now knows that it can no longer survive by saving energy. It is now directing all its energy to the most essential organs to keep the body alive. The timeline to death is hours to a few days. The breathing pattern has a more ominous significance when the caregivers observe it more frequently and lasting longer, with the pulse rising above 120 and the oxygen saturation falling consistently to the 80s.
I explain to families that when the heart, lungs and brainstem start to be adversely affected, the body’s path toward death progresses very quickly. One of the first observations are further changes in the breathing pattern. If the patient has been demonstrating the deep, regular Kussmaul breathing pattern, the family observes the breathing slowing down with less effort for a few minutes then restarting its forceful pattern for a variable time, then slowing down again. It is a strong sign that the body is running out of energy and that death is imminent.
If the brainstem remains in control of the path toward death, it will now distribute the body’s sparse energy to itself, the heart, and the lungs as evenly as possible so the body can continue to survive with good symptom control. When the patient is at this level, the objective observations are clear. The pulse is weak, often difficult to measure, often irregular or above 120 with oxygen saturation decreasing into the 70s and 60s or not measurable.
The approach to care when the kidneys, heart, lungs, and brainstem start to fail is to call the physician and nurse to discuss the findings and ask for an urgent assessment to quickly decide the next steps of care and symptom control.
The family begins to feel empowered when they understand the significance of the objective observations of pulse, oxygen saturation and the patterns of breathing as well as the significance of the subjective observations.
The introduction of a small, portable, battery-powered oximeter for the family’s use to measure their loved one’s pulse and oxygen saturation whenever they are worried increases their confidence to make simple decisions while awaiting confirmation of their findings by the physicians and nurses.