
My data demonstrated that patients diagnosed with kidney failure usually had a long history of slowly worsening kidney function. They were followed by physicians at hospital outpatient clinics specialized in kidney failure. At some point in their illness, investigations demonstrated a life-threatening decline in kidney function. Decisions were then made to start dialysis while awaiting a kidney transplant or to initiate a referral for palliative care. If a transplant was not possible, patients were given the choice to continue dialysis with occasional blood transfusions as needed, until both were no longer effective. At that point, the specialists made a referral for palliative care. These decisions ensured that patients participated in the decisions and extended their lives with the greatest quality but made the timeline from palliative care referral to death very short.
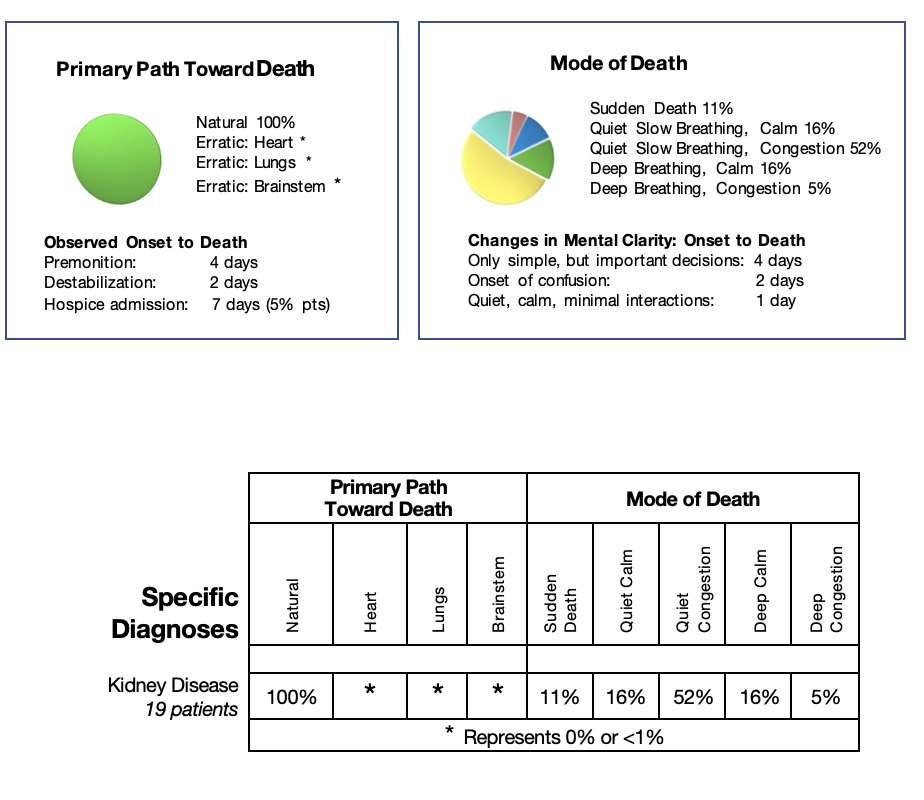
All my patients with kidney disease followed the body’s natural path toward death, but the timeline from premonition to death was much shorter than in patients whose path toward death was triggered by liver failure.
The mode of death was more varied. If the kidneys suddenly became non-functional, high potassium levels caused sudden death. If the kidneys were able to control the potassium but not able to remove the acid from the body, the brainstem initiated the Kussmaul breathing pattern. If the kidneys maintained a little of their essential functions, and the liver failed first, family’s observed weakness, sleepiness, and quiet slowing of breathing. If the heart was weakened through the kidney failure, lung congestion occurred requiring Scopolamine to dry the secretions and provide comfort.
Specific Diagnosis: Renal Failure
Natural Path Toward Death
Pre-referral Information:
Frederick, 90 years old, was diagnosed with chronic renal failure when his creatinine rose to twice the standard value over the last four years. He had been followed at the renal clinic of the Ottawa Hospital even though he had decided from the beginning NOT to have dialysis if his failure progressed. Frederick had signed a Do Not Resuscitate order. Three months before his referral to community palliative care, his creatinine doubled again. His physician told him that he was palliative, but Frederick did not understand why he needed a palliative care physician when he felt well. He had cared for his wife when she was diagnosed with cancer and ‘labelled’ as palliative. She had lived only three months. He ‘knew’ he had much longer to live.
Initial Contact:
Frederick reluctantly agreed to the palliative care referral. He had noticed some definite changes, including longer sleeping periods, over ten hours every night with frequent
naps during the day when reading. He ate about one-quarter of his usual meals. During my visit, Frederick led the conversation, looked comfortable and was not short of breath. His pulse, controlled by his pacemaker, was 55 and his oxygen saturation was 99%. Recent blood work demonstrated that his creatinine was now four times the normal. Still, his potassium was in the normal range. I asked Frederick his plans for near-end-of-life. He stated that he wished to stay at home until his death. His caregivers, including a neighbour in his apartment building, were willing to care for him. He was a veteran and had government insurance to help with any needed professional care. Frederick was eager to hear the answer to the questions “How long?” and “What will it be like?” I reviewed my Hierarchy of the Body card with him, his friend, and his power of attorney to explain his likely progression. He stated he would call me if there were any changes.
The Fusion of the Science with the Art of Near-End-Of-Life Care:
I visited Frederick and his power of attorney three months later. On review of his ‘world’ Frederick stated he was coping well. He now needed help with grocery shopping but could prepare his meals. His activity level and sleep were about the same. His vital signs were in the normal range. Frederick was mainly worried about his good friend, who had been hospitalized with a bowel obstruction, was now feeling better and was to be discharged in the next few days. He was worried about how he would care for her. He hoped she would agree to transfer to a retirement home for a few weeks to convalesce. If so, he would move with her.
I visited Frederick two weeks later. He was exhausted but coping well with many rest periods in the day. His friend had decided to return home after discharge, and she now had significant back pain making essential activities of daily living difficult. She and Frederick stayed at his apartment for evenings and nights and spent the days at his friend’s apartment. He was eating enough for his needs and his vital signs remained normal.
Another two weeks passed with no crises. Frederick found enough energy to go to the Remembrance Day Memorial service. He tolerated it well. It uplifted his spirits, and he became an instant ‘movie star’ at the service due to his age and his service to his country. He was tired for the next few days but recovered to his usual functional ability. He asked for another blood test – just to know how his disease was progressing. His creatinine was now five times higher than the standard value, with a normal potassium.
Premonition:
Two weeks before his death, Frederick’s power of attorney asked me to visit. He was observing some premonition signs. Frederick was more tired and eating less.
If he tried to eat more, he had sudden diarrhea. He admitted to more difficulty showering and dressing. Frederick appeared frail but could still walk about his apartment without shortness of breath. His vital signs remained normal. He was sociable, but his thinking was slower. He knew he was weakening and agreed to professional help for his essential daily activities in the daytime so he could remain at home.
Destabilization:
Over the next two weeks, we observed Frederick’s relentless steady destabilization as his body followed the natural path toward death.
Ten days before his death, Frederick could no longer eat and felt nauseated. I advised ginger ale and Gravol as needed. He settled and slept well. The next morning, Frederick reluctantly permitted his caregiver to wash him and help him dress. When she left, he tried to eat cereal which immediately caused diarrhea. I advised soups, toast, and jam only and ordered injectable medications and a foley catheter for the home to prepare for his future needs.
Seven days before his death, Frederick continued to weaken. He was now sleeping most of the day, eating and drinking very little. When awake, he would transfer to his chair and fall asleep again. He had no pain and no shortness of breath. His vital signs remained normal. He concentrated enough to explain his changes, understand the significance, and agree to all the help necessary to stay at home. We set up a hospital bed in his living room. The nurses inserted a foley catheter for his urine and established subcutaneous access for Nozinan, Midazolam, Hydromorphone and Scopolamine if needed for his comfort. Through his insurance, we set up continuous nursing care.
Five days before his death, all Frederick’s care was now in bed. He was nauseated when trying to eat, vomiting at times controlled by occasional Nozinan. His vital signs were unchanged, and his breathing was normal even after the stress of personal care. I ordered Nozinan every four hours regularly for the nausea.
Three days before his death, Frederick started to have periods of restlessness and confusion, always disoriented. Midazolam and Nozinan were helping to settle these episodes. He could no longer swallow, but he did tolerate mouth care well with sucking on the swabs for hydration. During my visit, he awakened, seemed to recognize me and stated, “I don’t know what is happening.” Although his vital signs remained normal, he now had a variant of Kussmaul breathing with deep regular breathing, not laboured and with no congestion.
Death Imminent:
One day before his death, I visited with Frederick, his son, the shift nurse, and his good friend. All were aware that Frederick’s death was imminent. He had remained quiet in the last twenty hours on regular Nozinan and an injection of Hydromorphone at bedtime. During the day, he required an injection of Midazolam before his care for comfort. Frederick appeared very comfortable. His pulse was 52 (I expected no changes due to his pacemaker). His oxygen saturation was 96%, with respirations at 20, no longer as deep with a short expiratory phase, demonstrating he had very little energy remaining. There was no need to change his medication regime. I supported Frederick’s friend and power of attorney and answered their questions. The following morning, after a quiet night, changes occurred suddenly. Frederick’s respirations increased to 24, very shallow with marked congestion, controlled with Scopolamine. His pulse was weak with irregular beats with an oxygen saturation at 84%. I explained that Frederick had just a few hours to live, and the nurses would ensure his comfort. Frederick died two hours later.
Frederick had lived a long life and felt at peace with the approach of his death. He was fiercely independent and wished to remain in control. He did enjoy his link with the renal clinic, not for any treatment, but to understand what was happening to him and to be able to predict, “How long?” Under my care, he asked for bloodwork three times, just to know how badly his ‘kidneys’ were working.
Frederick was not afraid of dying, nor of the process. He had cared for his wife at home. He had learned from the experience. His main concern, when he was demonstrating premonition signs, was how to care for his good friend after she returned home from her medical crisis. Together they both found a way.
When Frederick destabilized, he decided to accept all the necessary changes to care for his needs to be able to remain at home. Again, we followed his request, and he succeeded in dying quietly in his home with his power of attorney and his friend beside him.