
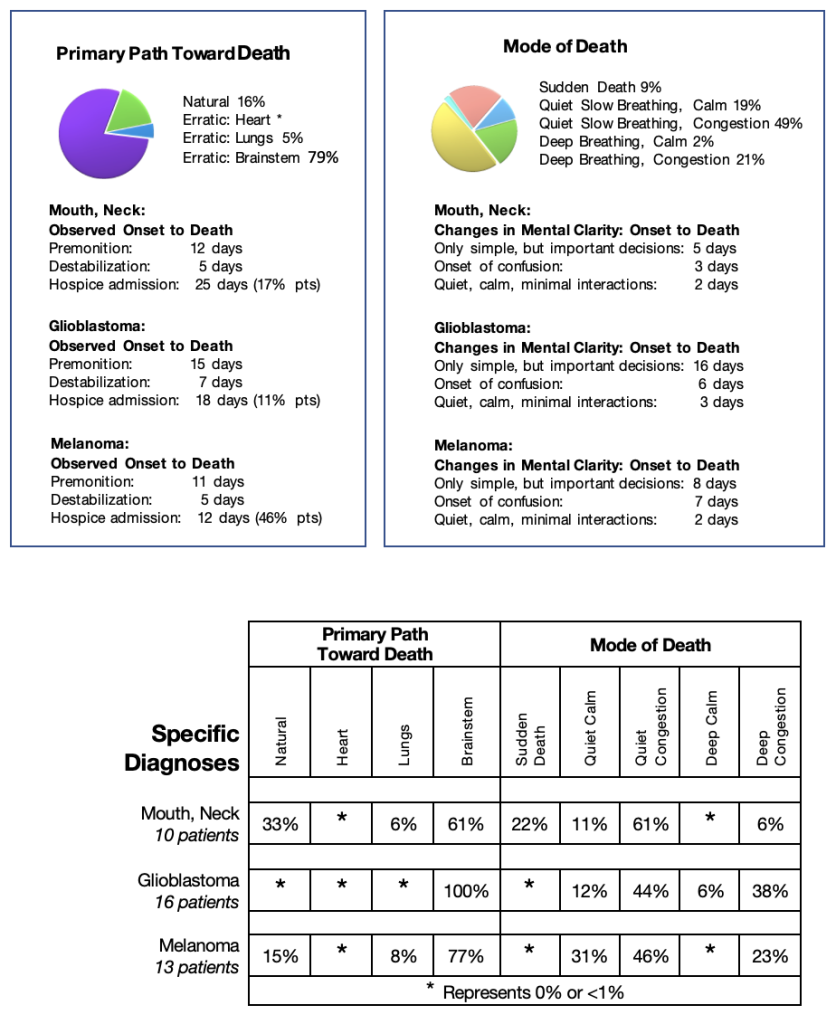
These three types of cancers were grouped together because most patients followed the erratic path toward death triggered by brainstem failure, a feature very different from the other cancer groups. Symptoms frequently included seizures requiring the regular use of Phenobarbital to control them.
Although the path toward death of head and neck cancers and melanoma were very similar near the end of their journey, the patients with each specific disease had very different symptoms at diagnosis and the early part of their journey. I chose to discuss their differences by reviewing each of these specific diagnoses separately.
Mouth, Neck Cancers:
The anatomical locations of head and neck cancers had the greatest influence in their spread. These cancers were close to major blood vessels to and from the brain, and in close proximity to the brainstem. If the cancer encased the blood vessels compromising the blood flow to the brain, or the cancer spread to the brainstem, the progression followed the erratic path toward death triggered by brainstem failure. Being adjacent to the esophagus of the digestive system, if these cancers spread locally and blocked the esophagus, the patients could not nourish themselves and followed the natural path toward death. Being also adjacent to the trachea, if swallowing was compromised causing aspiration of stomach contents into the lungs, patients followed the erratic path toward death triggered by lung failure. In the review of my data, none of the patients had erosion into the major blood vessels in the neck that would have caused massive bleeding and heart failure. However, this complication was a very real and frightening possibility.
Glioblastoma
Patients with cancer of the neural tissue of the brain, glioblastomas, did not experience spread outside of the cranium. Glioblastoma cancer cells spreading within the brain, caused two major life-threatening complications by increasing the pressure within the brain. They compressed the neurons and glial cells against the skull, interfering with the brain’s functions, leading to focal weakness, difficulty speaking, headaches, and confusion or they impeded the flow of cerebrospinal fluid within and around the brain leading to increased intracranial pressure and eventually brainstem dysfunction.
Increased Intracranial Pressure Leading to ‘Coning’:
Patients and families needed to understand the science of increased intracranial pressure caused by brain tumours before they faced this very frightening and often sudden complication. I started to explain the mechanics of the increased pressure, the expected symptoms and the significance of the changes before these crises occurred.
I started by describing the general structure of the brain, the production and functions of cerebrospinal fluid, and how the cancer spread impeded the flow of this fluid.
The brain, comprised of neurons and glial cells, and a series of reservoirs producing cerebrospinal fluid that are connected to narrow canals allowing the flow of fluid from deep within the brain to the brainstem, the spinal cord and over the surface of the brain. The cerebrospinal fluid, a clear, colourless fluid carries nutrients to the brain and spinal cord, helping to remove waste products and acting as a shock absorber. The cerebrospinal fluid is produced in the nighttime hours when the body is sleeping. If cancer cells block the canal system, the volume of cerebrospinal fluid increases pushing against the tissues of the brain toward the skull, then pushes the brain down into the brainstem, called coning, squeezing the brainstem towards the spinal cord and blocking its blood vessels, leading quickly to death if the pressure is not relieved.
The symptoms of increased intracranial pressure, usually start after midnight and continue to the early morning hours, often with symptom-free periods in the afternoon and evening when there is no production of the cerebrospinal fluid. The symptoms include headaches, nausea and vomiting, seizures, confusion, focal neurological signs, and decreased level of consciousness. The clearest premonition of this complication is the objective observation of a central pattern of breathing indicating the patient is starting to follow the erratic path toward death triggered by brainstem failure.
Melanoma:
Melanoma, originating from the skin, is usually diagnosed early due to the visible lesions. If the cancer is completely removed, with or without a course of radiation, the patient is cured. However, when melanoma recurs, it does so with a vengeance, experienced by the cancer seemingly exploding throughout the body, invading all the lymph nodes and organs. From my data, patients with melanoma did have spread in all areas of their body, but the life-threatening event was spread into the brain and brainstem, quickly leading to the erratic path toward death, triggered by brainstem failure. The likely explanation was that the brainstem space was very limited with a rigid cover. Intracranial pressure rapidly increased, leading to coning, and rapid brainstem failure.
Specific Diagnosis: Squamous Cell Cancer of Mouth
Erratic Path Toward Death Brainstem Trigger
Pre-referral Information:
Andrew was a 70-year-old man living with his wife in a two-story townhouse. He presented with a sore throat and mouth, enlarged lymph nodes on both sides of his neck causing progressive difficulty swallowing, and decreased hearing on the right side. He was diagnosed with a large lesion on the floor of his mouth, infiltrating into his tongue. He underwent local surgery, radiation, and a few months later, more extensive resection of his mandible, the base of his mouth and neck lymph nodes. Andrew did well for a year. Then, he developed a recurrence below the mandible. He was booked for an extensive surgical resection for palliation, not cure. The surgery was aborted when, during the operation, he suffered a cardiac arrest.
Initial Contact:
Andrew recovered and was discharged home under the care of his wife with twice daily nursing visits for his large facial and neck wound dressings. He was also referred for community palliative care. I was told on the referral that there was a significant complicating factor with the provision of his care at home. His wife, the primary caregiver, suffered from cardiac issues due to severe mitral regurgitation, limiting her physical abilities. She was due to have cardiac surgery in the next few months.
During my first visit to their home, in listening to the history and observing the couple, it was evident that both Andrew and his wife were overwhelmed with the reality of what was happening to them. They had accepted that Andrew had a recurrence of his cancer. They had adapted to the news Andrew would have a few years of good quality of life with the extensive surgery to his mouth and neck. But after he awakened from his surgery, Andrew and his wife were told that there was no further active treatment of his cancer, he now had a very short prognosis, and a community palliative care physician would care for his extensive wound and control his symptoms as his cancer progressed.
I quickly recognized the areas of care I needed to address and started to focus my questions. I asked how he was able to nourish himself. He explained that he was managing by taking protein drinks and soft food. He wanted to continue eating, but much of the fluid he tried to swallow leaked out of his extensive wound, creating the danger of seriously infecting the wound. He knew that very likely he would need a feeding tube soon. He had an appointment with his surgical specialist to discuss the feeding tube for nutrition within the next week. I asked about his pain. He stated that his pain was well controlled with a pump of Hydromorphone subcutaneously (equivalent to ½ vial every 4 hours). He tolerated the pump well.
I then shifted my inquiries and assessment to his very extensive wound. The surgery had been stopped after they had removed most of his right mandible, the right side of the base of his mouth, and part of his neck muscles. A passage had opened from his mouth cavity to beneath his chin. The wound was very clean. The area was healing, but changing the bandage was a complex twice a day procedure.
After my initial assessment, I really wondered if Andrew would be able to remain at home with his and his wife’s physical limitations. Andrew and his wife also had concerns that they clearly articulated. Andrew’s wife asked, “How can we possibly cope with this terrible wound, Andrew’s day-to-day personal care, his pain, and the functioning of this pump? And they told us that he would progress quickly. What will that be like?” Andrew had been prepared for major surgery and recovery. The cancelled surgery was merely a ‘bump in the road’ for him. He was still ready for the fight to recover, and he would do so at home. He ‘needed’ to recover to remove his wife’s burden of care and to take care of her. His question was, “How are you going to help me?”
After assessing this complicated situation, I did not think it would be possible for Andrew to stay at home for very long. There were just too many complex problems. But he had just returned home from the hospital, and as a couple, they were figuring out how they would proceed. They had to manage because Andrew was NOT returning to the hospital nor leaving his home! In the short term, I felt they could cope. Andrew was able to nourish himself, perform his essential activities and his pain was well controlled. He was tired but able to walk about his home on one level with a hospital bed on the main floor. He managed to climb the stairs once daily if needed. His vital signs were normal. Nurses were visiting twice daily, and he had close follow up with his hospital specialists for his surgical wound and discussions regarding the insertion of a gastric tube. I merely established a link with Andrew and his wife at the first visit. I set up a routine weekly visit schedule to monitor his wound and recovery from the surgery. The long-term goals would need to wait until we could assess how well he would recover from the surgery.
Wound Care:
Over the next few weeks, Andrew improved his functional capacity, performing most of his essential activities of daily living independently. However, the ulceration of his wound was expanding, an ominous sign. The chances of a significant crisis were increasing. I decided I needed to discuss his prognosis because the wound could progress quickly, triggering several crises. I explained to Andrew and his wife the body’s shutting down process and the possible complications for his specific disease, including bleeding from and infection of his wound and cardiac problems arising from his cardiac arrest during surgery.
We needed to keep the wound as infection-free as possible. Therefore, I discussed feeding alternatives, weighing the benefits of a feeding tube into his stomach versus oral feeds. The feeding tube was the easiest solution to prevent wound infection and for ease of administration. Andrew listened, thought about it and about a month later accepted a feeding tube insertion. The tube worked well with Andrew managing the feeds and cleaning the equipment independently. He soon found it easier to stop all his oral feeds. The surgical wound remained clear of infection, but the ulcerated area continued to extend, fortunately without significant bleeding.
The Fusion of the Science with the Art of Near-End-Of-Life Care:
Andrew was always tired but still tried to help with the chores in his home. His ability to remain home became more precarious as his wife’s condition worsened. During one of my visits, Andrew quietly stated, “I would like to get better! But that may not happen.” It was the first time he acknowledged realistically that he might not recover. Still, his pulse was 78 and his oxygen saturation was above 90%. He walked to the bathroom independently during my visit, but he was no longer managing the stairs. His other more significant concern was his wife’s cardiac problem. She was scheduled to visit with her cardiologist soon to decide the timing of her valvular heart operation. Andrew’s pain management was no longer optimal. He developed muscle spasms and drowsiness by the end of the third month, but he had no pain at the site of his wound. We wondered if he was progressing with the spread of cancer to his brain or receiving too much Hydromorphone. We reduced his Hydromorphone by half for a few days and were happily surprised when his functional capacity improved considerably, with his pain still in reasonable control. He tolerated an outing to a movie well.
By the middle of his fourth month at home, Andrew’s wound became more complicated. A part of his remaining mandible dislocated, opening a large hole from his chin to his mouth. He had more pain, well-controlled with a minor increase in the Hydromorphone. His speech was more difficult. His fatigue had returned. His wife’s valve replacement operation was booked for within two weeks. I needed to find a solution to provide care for Andrew while his wife was in hospital. I did not believe Andrew could remain at home alone at this point in his illness. We needed to make use of all the community resources possible, even if not in conventional ways.
I spoke with the nurse coordinator at the residential hospice to request admission for Andrew. We discussed the issues around the progression of his illness. He had been home for over three months, he was weakening, sleeping most of the time, had swelling of his limbs, and require a decrease in his feeds. His wounds were progressing, causing more pain and less ability to communicate, his hands too shaky to write.
He could barely transfer, still his vital signs were normal. I explained my request for admission. I thought there was a good chance he was starting to destabilize and would need symptom control as he continued to progress. But I added that if he stabilized after his admission to hospice, I would request a respite admission for six weeks while his wife underwent mitral valve replacement and convalesced. I reassured the hospice team that Andrew would NOT stay at the hospice if he was stable, and his wife returned home after her operation.
Andrew was admitted to the residential hospice a few days before his wife’s surgery. All the team members at the hospice felt the admission was appropriate even though Andrew did all his care independently, handled his feeds via the feeding tube and cleaned the equipment. His wound demonstrated how fragile he was. None of the team members had ever seen such an extensive wound of the mandible, mouth, and neck. They were amazed that Andrew was still functioning well and frightened of the complications and care it would require. The gaping area of his right jaw was dramatic – all the caregivers could see directly into the back of his throat!
Andrew worked with each of the nurses to help them care for the wound and teach them how to apply the dressing correctly. He always participated in the dressing change to ensure every detail was done according to his specifications. After a few weeks, the nurses and Andrew started to trust each other and improved the routine making the time-consuming wound care easier and the dressing more comfortable. Eventually, Andrew had enough confidence to let the nurses do the procedure without his help. Every few days, the nurses, for reassurance, would ask me to reassess the wound. I agreed that the erosion was extending but the wound remained very clean and infection-free, and the erosion edge had enough fibrous tissue to prevent significant bleeding. During his entire stay at the hospice, Andrew required only one intervention for increasing pain in that area. We doubled the Hydromorphone from the pump with good effect.
Although Andrew wished to do all his care independently (because, of course, he was confident he would be going home soon and would need to be independent with his care needs), the nurses found ways to make his care easier and reduce his need to waste his precious energy. Andrew stabilized and realized he was able to do more important activities. With volunteers or family, he visited his wife at least twice weekly at the hospital cardiac unit and then in the convalescent care. His wife had a significant complication with heart failure soon after her operation, requiring more time to recover at the long-term care facility.
The hospice team agreed to extend Andrew’s care for another four weeks to allow his wife a smooth transition to home. The Home Care coordinator set up nursing shifts for eight hours daily for two weeks when she was discharged home. Hospice volunteers brought his wife to the hospice once weekly. Andrew and his wife spent time in the garden, played board games, and watched TV together. After ten weeks, Andrew was discharged home. This wife was coping well, though still very fragile. All the services and equipment were in place. When I visited his home Andrew was delighted to be home and looked well. His vital signs were normal. He had mild swelling of his lower legs and feet. His pain was under control, his feeds and bowels were working well. I left an oximeter in the home, so he and his wife could monitor any changes that could predict a crisis.
Andrew went back into his caregiver mode. He was determined to remove his care burden from his wife and help her recover from her surgery. He decided he had more energy than his wife to climb the stairs. Therefore, he gave his hospital bed on the main floor to his wife and used his bed on the second floor each night. They coped for the first month with no significant problems. One month after Andrew returned home, his wife developed pneumonia and was admitted to the hospital for one week. Andrew was now home alone. He started to progress within a few days, mainly with increasing fatigue. He stopped using the stairs and slept on the main floor. His vital signs remained normal, with no change in his feeds and bowels. His mentation was clear, communicating by writing. Andrew’s wound continued to extend, but the bandage routine remained the same. His pain in that area was more severe, but Andrew was reluctant to take extra Hydromorphone because he felt it caused drowsiness and muscle jerks. He agreed to pace his activities, to rest for an extended period in the afternoon and to adding a small pain patch to his regime as a simple way to give him a little more pain relief. A week later, I arrived at his home just before Andrew returned from a grocery trip, walking carrying a heavy bag of vegetables. His vital signs remained normal with the effort. He felt that the pain patch was controlling his pain.
Ominous Premonition:
Andrew’s wife recovered from her pneumonia and returned home. For several weeks, they continued to cope by themselves. Then I observed changes indicating an ominous premonition that Andrew was progressing, but I felt changes were not life-threatening yet. He began to have recurring shooting pains in his head, often after the effort of have a bowel movement. His wound changed with his lower lip pulling apart, his cheek swelling. There was an odour of infection within the erosion, but no bleeding. Still, he was thinking clearly, his vital signs remained normal.
I knew from experience that in patients with head and neck tumours that Andrew’s destabilization would most likely follow one of three paths. His cancer could extend locally, eroding into a major blood vessel in the neck leading to a severe, life-threatening bleeding episode or the wound could become infected. Also, without symptoms, the tumour could silently extend into the nearby brainstem. Andrew was at significant risk for all three of these complications, all of which would cause very rapid deterioration to death. I had to monitor him carefully to catch the more life-threatening premonition symptoms as early as possible. For the present moment, I needed to address his headache that was interfering with his rest and activity. I added a small Phenobarbital dose at bedtime and decreased his feeds and activity in case the headache was a symptom of increasing pressure in his brain.
A week later, there were more signs of progression, still not life-threatening. Andrew was more tired, and now he admitted he was sad that he could not do more. He agreed to a walker to steady himself while going for walks. He was still managing the stairs daily. His vital signs remained stable. He was sleeping better with the Phenobarb but now had occasional bouts of shooting pain in his right cheek controlled by boluses of Hydromorphone. His wound had a greenish odorous discharge, likely infected. We added an antibiotic cream to the dressing protocol. I still could not identify his destabilizing path toward death. I felt he could still stay at home for now.
Destabilization:
Two weeks before Andrew’s death, it became evident that Andrew was following the erratic path toward death, triggered by brainstem failure. He was sleeping most of the time, but he had some lucid periods. He took short walks and tolerated reduced feeds. I ordered day shift nursing to help keep Andrew at home.
One week before he died, Andrew slept except for feeds and medications for two days, then the next day he was more awake.
Two days before he died, Andrew had a crisis with confusion, restlessness and walking about the house at night. His wife was exhausted, crying, feeling she could no longer cope. I requested an urgent admission to the hospice.
One day before he died, I observed Andrew walking from a nearby gas station with his walker towards his home. He succeeded but was very confused on his return home. His wife stated he walked daily to the gas station to buy copious lottery tickets. His wife worried that he would spend all their money. He was admitted to the hospice by that afternoon.
Death Imminent:
Andrew’s rapid destabilization began the morning of his death. He developed congestion, a pulse of 144, and a high fever. His oxygen saturation was 77% with gasping respirations. He had minimal response to any stimulus. I stopped his feeds, added Scopolamine to his medication regime and increased his Phenobarbital to twice daily. By the afternoon, Andrew was calm, not responding, appeared very pale, dusky, and had an oxygen saturation of 51%, a pulse of 160, and gasping respirations with less effort. His family was at his bedside. He continued to weaken and died quietly the same evening.
Andrew was a very proud man, a loving husband. He faced his problems directly and formulated a plan to overcome them. When faced with the news of progressing cancer that could no longer be treated, he decided to return home to take care of himself without burdening his wife. He was also determined to care for his wife until she recovered from her cardiac surgery and could live independently. And Andrew succeeded!
Out of love for his wife, Andrew agreed to a respite admission to a residential hospice.
When she came home, he returned home as well, for himself, yes, but mainly to take care of his wife. By sheer willpower, he found the strength to care for her until she recovered enough to be able to stay home independently when he could no longer be with her.
As the tumour was invading his brainstem, causing confusion and destabilization, he had one more task during his lucid moments. I believe he knew he was dying and wanted to help his wife financially by winning a jackpot with the lottery tickets.
When that did not work out well, the day before he died, he quietly accepted admission to the hospice, again to protect his wife, giving her the support of the hospice staff, when she held his hand as he died peacefully.
(Based on a true journey)
Pre-referral Information:
Eric, 69 years old, presented with a short history of increasing confusion and difficulty finding words. An MRI demonstrated a large mass in his left temporal lobe. A biopsy confirmed a high-grade glioblastoma. His tumour was partially removed, followed by radiation and a course of oral chemotherapy. Two months after his active treatment was completed, he presented to the hospital with confusion and incontinence of urine. Investigations were inconclusive for recurrence of his cancer.
He was treated for a urinary tract infection, returned home, and stabilized. Four months later, he developed seizures. Again investigations, including MRI, did not demonstrate cancer progression in his brain. Still, he was referred for community palliative care for symptom control and near-end-of-life care at home.
Initial Contact:
I first visited with Eric, his wife, and his children at home. His wife provided the history while Eric listened. She explained that Eric was stable functionally. He nourished himself with smoothies and thickened fluids, having difficulty swallowing mainly in the mornings. He was sleeping well. His seizures were controlled with a slight increase in his anti-seizure medications. Still, to maintain this stability, he needed a high dose of the steroid Decadron.
On my review of his history, present condition, and medication regime, I was more concerned about his precarious situation than his wife. Indeed, Eric died within two weeks of my first visit.
My greatest worry was his increased intracranial pressure. I knew that it was still high because his referring physicians had prescribed a high dose of Decadron to control it. Over time, he would develop major side effects from such a high dose. As well, Eric was on intravenous hydration even though he was able to nourish and hydrate himself oral, increasing the chances of aggravating his increased intracranial pressure. We discussed my concerns and decided to stop the intravenous hydration but keep the Decadron at the same dose for a week and monitor his symptoms. If he remained stable, I suggested that we slowly decrease the Decadron every week, carefully monitoring the effect to help prevent side effects and objectively determine if his tumour growth was controlled. Eric had suffered several urinary tract infections treated with antibiotics. Whenever the antibiotics were stopped, the urinary symptoms recurred. We decided to continue the intravenous antibiotic indefinitely. Eric seizures were controlled on his present medication regime, so we did not make any changes except to ensure that Midazolam was present in the home in case of a sudden seizure episode.
Eric’s goal was to stay at home. He had a Family physician who wished to participate in the ongoing care with me jointly. We all agreed to that arrangement. I contacted the Home Care Coordinator to set up daily shift nursing to help with Eric’s care and medications.
I visited with Eric, his wife and daughter, with the shift nurse present two days later. Eric had stabilized with the extra care at home and the simplified medication regime.
He had no pain and slept well. He was very drowsy in the morning but more awake in the afternoon and evening, able to answer simple questions. Eric could still hydrate and nourish himself with soft food, though, occasionally, he coughed from food residue in his mouth. His breathing was a Cheyne Stokes pattern, not laboured or congested, with an oxygen saturation of 97%, pulse 84. He was comfortable but precarious. I asked the family about their goals of care in greater depth. They confirmed that they would care for Eric at home. We reviewed and signed the DNR document. Together, we decided to keep the same medication regime. I ordered a suction machine to remove residual food from his mouth and supplemental oxygen in case of shortness of breath in the future.
Premonition:
Five days before Eric’s death, during my visit, his wife reported that he had not eaten for 24 hours and could barely take his oral medications. Eric also had episodes of coughing and some restlessness controlled by occasional injections of Hydromorphone and Midazolam. He appeared very comfortable and responded to my gentle examination. His respirations and oxygen saturations were normal.
I explained to the family that these observed changes were premonitions, not life-threatening yet, but indicated that Eric’s cancer was progressing, and he might die within one or two weeks. The family could not believe he was so close to dying – he was still eating, drinking and participating in conversations. They asked me to increase his dose of Decadron to resolve the new changes, as this approach had worked before. I agreed to the trial.
Four days before his death, Eric was a little better in the morning, awake enough to take his anti-seizure medications and Decadron orally. Still, by the evening, he weakened again. He coughed with any fluid and medications. His oxygen saturation was about 80%. The family saw for themselves that Eric ‘was’ progressing and agreed to stop his oral medications, switch to Phenobarbital intramuscularly for his seizures, and continue Hydromorphone for cough and Midazolam for restlessness subcutaneously as needed.
Destabilization:
Three days before death, Eric was comfortable. He had required only one dose of Hydromorphone for cough overnight. Still, he was barely responding to voice or touch, with oxygen saturations in the mid 80%, pulse 90. Eric’s respirations had changed to rapid, deep, and regular, a Central pattern, objective evidence of increased intracranial pressure. His lungs were on the edge of congestion, and he had several focal seizures in the morning. Eric’s family and I discussed the significance of the changes.
Eric now demonstrated life-threatening signs of destabilization, with a prognosis of hours to a few days. His family had observed the changes and now believed that he would die within a few days. Their goals of care became ‘his comfort above his wakefulness’. We increased the Phenobarbital to twice daily regularly to control his seizures, and added Scopolamine subcutaneously as needed for congestion.
Death Imminent:
Two days before his death, I reassessed Eric. He had settled with the new medication regime. His night was very peaceful. The family was very pleased that he was still responding to voice. During my visit, he had no congestion, much less coughing, but he was not awake enough to drink. His vital signs remained unchanged.
One day before his death, as night approached, Eric remained comfortable but deteriorated rapidly, the typical pattern of increasing intracranial pressure. His respirations remained rapid but now he was too tired to breathe deeply. His pulse weakened, with a rate 116. His oxygen saturation dropped to 85% on supplemental oxygen. He restarted mild congestion. He stabilized by the following morning but did not improve. In discussion with his family, I explained that the same cycle of progression would happen as night approached, but that this time, he would be too weak to survive through the night. We started Scopolamine and Midazolam regularly every four hours for his comfort. Eric remained very quiet during the day and died peacefully with his family at his bedside just after midnight.
Eric’s journey is characteristic of a person diagnosed with a glioblastoma. Initially, a patient presents with sudden changes in mentation, headaches, or seizures. Investigations demonstrated cancer deposits within the brain. Surgery, radiation, and chemotherapy are initiated quickly with initial improvement. Then, there is recurrence with rapid deterioration that is very challenging for patients and families to accept.
It is essential to explain to the patient and family what they are observing and the ‘science’ underlying the symptoms as early as possible because the deterioration can be rapid following the ‘erratic’ path toward death. They must be prepared for these changes.
It is also essential to add ‘art’ to the approach of care by carefully observing the patient’s and family’s responses to the changes and together finding ways to stabilize the symptoms and build trust. Improvement may be for only a short time, but the fusion of the art and science will allow the family to understand and enhance their loved one’s quality of life.
Pre-referral Information:
Brian was a complicated man. He was a retired high school science teacher. He had obsessive-compulsive tendencies translating into a character that demanded order, punctuality, and attention to detail. After retirement, he became a super athlete, mainly in cycling and skiing. He hated any medication that would interfere with his physical and mental prowess. Brian was divorced but maintained a good relationship with his wife, who unfortunately lived in western Canada. He lived alone in an apartment complex on the third floor with no functioning elevator. All the laundry facilities were in the basement. He had deep connections with his church, and many members provided significant support for him through an outreach program.
Initial Contact:
I was first involved in Brian’s care late in his illness (from the point of view of the referring physician but not from Brian’s point of view). Brian had been diagnosed with malignant melanoma with extensive spread to his liver. He had undergone all possible treatments except for an immunotherapy trial in the USA. The referring team did not feel experimental treatment would be beneficial, but Brian held some hope. Brian was still feeling quite well when we first met and was not happy to have been referred to a palliative care physician. He cancelled our first meeting because I was thirty minutes late, and he had things to do (i.e., go grocery shopping on his bicycle). He reluctantly agreed to set up another visit. I made sure I arrived on time at the next meeting. I pressed the ringer code, but the door did not open. He ran down three flights of stairs to open the door, said hello and then raced up the three flights while I struggled to climb the stairs with my heavy medical bag.
I, too, began to feel there might be something wrong with the timing of the referral. It was not difficult to obtain a history from Brian. He quickly and concisely told me his story. Then he stated he had only three symptoms. Brian described a nerve pain, likely a side effect of the chemotherapy. The pain was tolerable with regular Lyrica and small doses of long-acting Hydromorphone, he did not wish any changes. Brian was anxious and not sleeping well, helped a little with an occasional Lorazepam. He did not wish to make any changes worried about drowsiness in the day. Fatigue was Brian’s primary concern. He had his usual functional ability inside his apartment, but outdoors, fatigue was interfering with his cycling and grocery shopping.
My assessment of the issues was very different. Brian had very extensive melanoma in his liver despite appearing so well. He would likely quickly slip into liver failure.
But I could not address these issues due to Brian’s present state of mind. He still held out hope for immunotherapy treatment in the USA. His pain was adequately controlled. Any treatment with medications for his anxiety would likely make him sleepy in the day and interfere with his activity, so I could not start there.
Approach to Symptom Control:
I decided to start building some trust by addressing Brian’s primary concern – his low energy level. For Brian, the fatigue was very distressing, interfering with his cycling (Even though he admitted he still had 90% of his energy.) I offered a trial of a tiny dose of Decadron daily, hoping it would not increase his anxiety but help his energy level and decrease his need for Hydromorphone. If it did nothing for his fatigue, I would know more clearly that he had little reserve energy and, therefore, a short prognosis. Perhaps then, we could talk about important issues about his care needs and goals during his near-end-of-life. After a week, he admitted the Decadron did help a little but not as much as he had hoped. The following week, he was even better. He asked me not to call him. He would call if he needed help.
Two months later, Brian called to let me know that he was feeling much better, was leaving for a ski trip in the Kananaskis for two weeks. On his return he stated he had a wonderful time skiing every day. Because he was so well, he had stopped the Decadron because it made him feel more anxious. He was about to go to Rochester for the experimental treatment. He contacted me the following week. The planned treatment in Rochester had been cancelled because an MRI revealed progression of his disease. Brian was now interested in a trial of chemotherapy requiring a trip to Toronto every two weeks. I felt Brian’s condition was quite precarious, and he would soon need my help with symptom control. But he was still in an ‘active mode’ for treatment and very hopeful. I explained that I would stay in the background for advice until he had exhausted his active treatment options. Over the next six months, Brian had crisis after crisis but was still pursuing his treatment options. Surprisingly, he would call each time he was concerned about a new symptom including jaundice caused by a blocked bile duct, and high fevers caused by severe infections. I gave advice each time, mainly explaining he needed to go to the hospital or contact his oncologist for further assessment.
Premonition:
Brian did not return to baseline during his last admission to the acute care hospital. He developed an agitated confusion with high ammonia levels, increasing jaundice, and anemia.
He settled somewhat with treatment, but his jaundice continued, his agitation with aggressive behaviour was difficult to control, his functional ability decreased, and he had increased pain and hiccups. To my great surprise, Brian called me from the hospital. He was panicky, on the edge of confusion, but could communicate very slowly and coherently with me. He wanted a transfer to a community hospice under my care. His nurse did not feel a transfer to hospice was possible due to his aggressive, confused behaviour and his very short life expectancy. However, the attending physician asked if I would evaluate Brian at the hospital and consider the transfer.
Fusion of the Science with the Art of Near-End-of-Life Care:
I visited with Brian, his ex-wife, his church minister, and his power of attorney. With difficulty, frequently stopping for very distressing hiccups and spasms in this back, Brian explained his wishes. He wanted to transfer to the community hospice and be under my care. He understood that he must agree to DNR, no intravenous antibiotics or other intravenous medications except for the pump for pain control. He would continue subcutaneous and oral medication to control his confusion.
In front of his trusted witnesses, I explained I would agree to the transfer under my care if he understood that I would ultimately determine the medication regime. Yes, we would find a medication routine to keep him the most comfortable, address his confusion, hiccups, and pain, and try to keep him as mentally clear and as awake as possible in the day. I would explain and discuss the regime with him. But I would make the final decisions. He looked deeply into my eyes, thought about it, and said, “You are asking me to take a leap of faith.” I replied simply, “Yes, I am.” And he agreed to all the terms.
I negotiated with the hospice staff, explaining Brian’s history, the symptoms and the rules Brian would follow when admitted. I said if Brian did not follow the plan, both Brian and the hospital had agreed he would be transferred back to the hospital. Brian was admitted to hospice a few days later. On arrival, he was alert, a little restless, on the edge of paranoia and confusion, but cooperative and happy to be at the hospice. His pulse 75 and oxygen saturation 98% remained stable. His abdomen was distended with an enlarged liver and ascites but not tender. He had mild jaundice. I felt, with all the crises in the last few months, his lack of improvement in the recent hospital admission and the assessment of the hospital team, that he was likely at near-end-of-life.
I needed to keep that in mind in setting up his care plan. I needed to use my science knowledge and incorporate the art into Brian’s care – this was not going to be easy. He needed consistency in his care. His medication regime had to be the simplest possible
with the fewest injections but had to include regular antipsychotic medications whose route of administration could be changed to injections.
Pain:
While Brian was in the acute hospital, the staff felt he was a drug seeker demanding too much Hydromorphone for his pain level. But from my experience with Brian, I knew he was NOT a drug seeker. I felt part of Brian’s confusion, and his frustration was that doctors and nurses did not believe him when he reported severe pain. I did not doubt Brian had enough pain to merit a continuous infusion of Hydromorphone. Brian had central tubing for intravenous medication. I ordered a pump to deliver a continuous baseline dose of Hydromorphone, the same dose he had been on orally pre-admission and allow him a self-controlled bolus dose intravenously. On this regime, using very few extra doses, Brian’s pain remained well controlled throughout his stay at the hospice.
Confusion:
Brian remained on the edge of confusion. We ‘controlled’ his confusion, but never ‘resolved’ it. We tried to give him the best control with the most negligible sedation in the day and a quickly available ‘rescue’ medication if he suddenly became very aggressive.
Brian, contrary to everyone’s expectations, quickly improved. I observed him walking slowly but independently in the halls within a few days, eating a full meal with appetite. His mentation started to clear. He tolerated a shower and asked for his friends from the church to visit him. He started to request a decrease his medications. I knew Brian would begin to think about going back home. I knew we were going to face a crisis soon from two directions. Although Brian still had some jaundice, he was walking about and eating well for someone with liver failure. The hospice staff was starting to wonder if Brian was appropriate for the near-end-of-life care at the hospice. Brian, himself, was more and more convinced he was not dying. He benefited from the care and support of the staff and his church. His pastor organized a communion service in a quiet room on the unit, he attended the day hospice. Brian and has wife decided she should go back to her home in British Columbia and return in the future as needed.
Finding an ‘Elegant’ Solution in Brian’s Care:
By the third week of Brian’s admission to the hospice, he continued to improve, so I decided to pre-empt the next crisis. I discussed with Brian and the staff about a trial of going home initially just for a visit and a trip to the bank for his finances with the help of his church outreach volunteers. I reminded Brian that his apartment was on the third floor with no elevator. I challenged him as an athlete to start to build up his stamina by walking about the garden at the hospice, in a rational, paced manner so as not to cause a setback by doing too much too soon. I told him that I would give him a pass to go home for the afternoon once he achieved the physical ability to walk about the entire circumference of the hospice gardens three times without stopping.
He took up the challenge enthusiastically, and within two days he had achieved the stamina criteria. At the beginning of the fourth week, Brian went out to his apartment, managing the stairs without problems. Then he decided to go for blood work, then a meal and finally a trip to the bank. He tolerated the whole trip very well. The next day Brian was well and eager for more activity. Before he asked, I told Brian we should start to make plans to go home for as long as he had the strength, making sure he had all the community resources in place to help him. Brian ‘beamed’ – very pleased and very cooperative! I hoped that Brian could stay at home for at least a week. If we could achieve that goal, all the effort to get Brian home would be worthwhile. Even being home for a few days would be a success for Brian. I knew the project would need superb coordination.
It took a week to set up the logistics of his care at home. Brian was familiar with and trusted two nurses in the community who had followed him through his chemotherapy. We ensured that these two nurses were the only ones who visited four times weekly to assess his symptoms, care for his pumps and set up his other medications. I would do the home visits the other three days to do the nursing tasks with the pumps and drugs and assess any impending crises. If the nurses needed my help, they had immediate access to me by phone. Brian had access to me 24/7 by phone. A personal support worker (the same one) would visit twice weekly: one visit for laundry and one visit for personal care. She would always be the same person, who did exactly what he asked. Members of his church group would visit at least once weekly to take Brian for banking, shopping and to support him. Quickly they noticed Brian could not manage the stove and bought microwave dinners. A volunteer from the hospice would bring Brian to Day Hospice and back home weekly. I knew I needed to make Brian’s medication regime as simple as possible. He did not like change, so we essentially kept the same regime as in hospice, the nurses or I set up the daily regime with each visit.
Brian was discharged home after six weeks at the hospice. I received no panic calls for the first few days. With each visit, we observed that Brian could cope at home, but the balance was precarious. On the positive side, Brian could walk about his apartment, use the stairs, take his medications easily, and cope with his two pumps. Yes – Brian was going to manage at home – but for how long? As the best outcome, we had expected that Brian would stay at home for a week before destabilizing.
And yet again, Brian continued to surprise us! He managed to stay at home for a full six weeks. There were no significant crises and no need to change his medications. He was able to go out with his church friends and did not miss a week at day hospice. He called me with minor problems with his pumps only a few times.
Premonition:
At the beginning of the sixth week at home, Brian appeared more tired. He was able to talk about his symptoms calmly. He explained he would not be able to stay at home much longer because although he was still eating, he had no appetite, his walks outside were shorter and his recovery time longer. Amazingly his vital signs remained normal. A few days later, the visiting nurse contacted me. She was with Brian, who was not well. She had given a bolus of Midazolam. I asked her to administer a bolus of Hydromorphone as well. When I arrived, Brian was feeling a little better. He had been very concerned with heaviness on his chest and difficulty breathing. He could still walk about slowly in his apartment with no evident shortness of breath. His oxygen saturation was in the low 90s, not dangerous but much lower than usual for him. He came to me and put his head on my shoulder, saying, “I can’t do this anymore; I need to go back to the hospice.” I called the hospice staff and asked for urgent admission. The volunteers from the church stayed with Brian each night to ensure there would be no crisis until he was readmitted a few days later.
The Benefit of Hospice Care:
On admission to hospice, all the nurses and personal support workers remembered Brian and observed how very tired and weak he appeared with increased jaundice and large lymph nodes in his neck. Brian remembered the nurses. His mentation was slow, but he interacted well. He was relieved to have the support of the nurses and was very mellow about coming back, stating, “I am surprised, I am too tired to be angry at anything.” We did not change his medications from home except to offer him an extra Nozinan dose at bedtime and encouraged him to use the bolus of Midazolam and Hydromorphone liberally in the night if he was uncomfortable. His vital signs were stable. He could still visit with his friends.
The next few days were a real ‘wake-up’ call for Brian. I think he believed if he came back to hospice with all its support, he would recover back to his baseline as he had done during his first admission. I explained that he would likely have good days but would need to rest after any activity and learn to pace his activities. A week later, his ex-wife returned to Ottawa and helped alleviate some of his fears and paranoia. By then, he was even weaker, his confusion increased, and he was only able to walk short distances.
Destabilization:
Two weeks before his death, Brian could no longer go to the day hospice. However, he had completed six drawings of locations visited on his bicycle rides. The staff quickly worked to get them all framed. Brian wished to give these back to the hospice to thank all the team for the help they had given him. He was eating less, more fearful at night, more upset with any attempt to change his medication. With the swelling in his neck, he had more difficulty swallowing and taking his oral medications. And if asleep at the time of his scheduled drugs, he became angry if he was awakened. I needed to find a solution for his Nozinan, the essential medication to prevent the recurrence of his agitated and aggressive confusion. Soon he would not be able to swallow, and the subcutaneous injections caused irritation of his skin. I discussed the administration of Nozinan with the pharmacist. We knew that Hydromorphone and Nozinan could be mixed and likely would remain stable for a few days. We combined the Hydromorphone and Nozinan in appropriate concentrations in the same cassette and gave both drugs continuously by the pump, monitoring closely. Fortunately, the trial worked very well and controlled his confusion.
One week before his death, we stopped all his oral medications, continuing his Phenobarbital at bedtime by injection. I increased his baseline and bolus dose of Midazolam. As he weakened further and could not swallow, we changed his Phenobarbital to an injection twice daily to improve his sleep at night.
Death Imminent:
A few hours before he died, Brian started a Kussmaul breathing pattern, demonstrating he was now in renal failure. He became congested, with his oxygen saturation falling to 70%. We added Scopolamine subcutaneously regularly every four hours. He remained comfortable. He died quietly through the night with his wife beside him.
Brian was very independent and very proud of his mental and physical abilities. He had difficulties with social interactions, but his friendships were lasting and very important. He tried very hard to communicate his gratitude for their friendship. He loved life and was not ready to give in to his disease even at his near-end-of-life.
To help Brian with the progression of his illness and his symptoms, we needed to understand these unique aspects of Brian’s personality. He would listen carefully to the information and advice given to him, evaluate the validity of the advice and then do what he wanted.
When many physicians and nurses gave Brian a poor prognosis, Brian worked hard to prove them wrong and, to our surprise, often succeeded. He stayed home independently and continued many of his physical activities so much longer than anyone would have predicted. When the medical team at his last hospitalization predicted he would die within a few days, after six weeks in the residential hospice, he succeeded in returning home independently for another six weeks.
During the last sixteen weeks between hospice and home, he fought to survive, but he knew in his heart that he was dying, and he prepared to find a way to thank those important to him. He was able to go to his church with two intravenous pumps and stand before the members to thank them all for their help. He participated in Day Hospice weekly, drawing and painting pictures of scenes significant to him of places where he had cycled. He offered them to the hospice to be auctioned off. He gave his ex-wife permission to return to her home in British Columbia to continue her life, asking her to come back only for the last few weeks to help him in his final journey.