
With my university background in research and experience in clinical research, I knew the importance of demonstrating the validity of my approach to near-end-of-life care.
I evolved my teaching card, as demonstrated by the series of graphics, each with a summary of what patients and families could review at a quick glance (Chapters 18-21). Verified by years of clinical experience in caring for patients at near-end-of-life, I believed in the information, but did not have objective proof that my summaries were accurate.
Throughout the last nine years of my community practice, I collected clinical data from each patient visit onto a digitalized database. In partnership with my brother, we developed a computerized patient database specific to the care of patients at near-end-of-life, ready for use when I started my new solo near-end-of-life community practice in 2010. Our software release coincided with powerful and easy to access digital connectivity – a key element for success. We found the appropriate hardware, a tablet capable of linking to the internet and a light-weight portable, battery charged printer linked to the tablet, so that I could carry my ‘files’ to each patient home and leave a printed copy of my notes at the home. The Ottawa Palliative Home Care resources included a clinical ‘Chart in the Home’, binder into which all the care providers were required to enter their visit notes. I developed a simple method to print every visit note into the binder, sequentially with the other care providers, during my home visits.
I used a methodical approach to writing my notes, called the SOAP method. It followed the same sequential approach I used in discussions with my patients and families:
By the time I left each patient’s home, my notes were within the reach of patients, families, and all the other care providers. I retained access to the same information on my computer no matter where I was in the city.
These notes were essential for my day-to-day practice. Also, when I retired and was ready to review and validate my approach to near-end-of-care, the information remained easily accessible.
One year after I started my Near-End-Of-Life community practice I agreed to a College of Physicians and Surgeons of Ontario peer assessment of my medical records and clinical practice including a discussion with the assessor. The peer assessor reached a favourable conclusion about my record-keeping and clinical practice, accepted without further scrutiny by the Committee. By this assessment, I felt validated in my methods of providing community near-end-of-life care and my data collection program.
Over the next nine years, I continued to use this approach to care. Together with my patients and families, we fused the science of near-end-of-life with the art of each family’s unique history, needs and goals for their best quality of life. Throughout the process, quietly in the background, I collected the real-time clinical data I would need to validate this care for each individual.
General Review of the Clinical Data
After I retired in 2019, I started to review the digitalized clinical data of each of my patients, choosing the last 1000 patients for whom I was the most responsible physician. The process took over two years. The initial review of the data was broad and simple, meant to answer three basic questions.
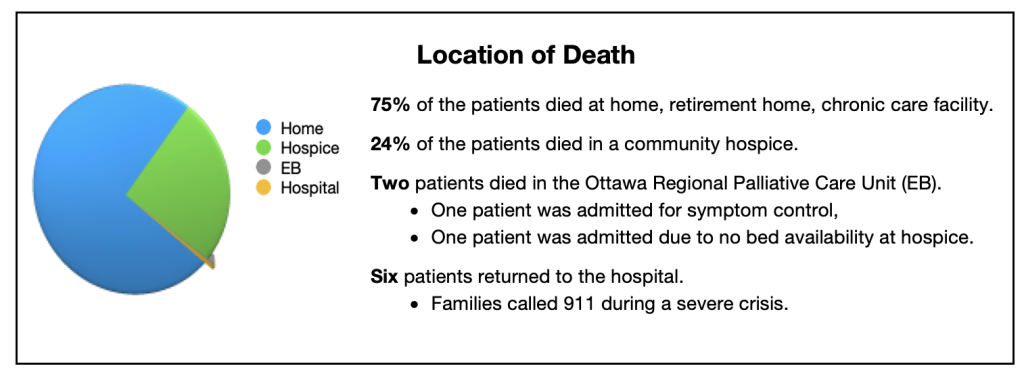
My criteria to answer “Yes” to this question would require supporting data that I achieved my primary goal to provide care for my patients and families until their death at home, a residential hospice or at their ‘perceived’ home within a retirement home or a long term care facility. Even I, who provided the care, was surprised that the data verified 99% of the patients in my study group died in the community under my care. The chart below depicts this evidence by location of death.
When I first started my community practice, twenty three years ago, most of my families did not want me to discuss dying in front of their loved ones. Over the years, I noticed a shift in their thinking toward asking to understand the process better. When I started my near-end-of-life community practice, I assumed that all patients and families now wanted to understand the significance of what was happening and be involved in the care decisions. I asked patients and families at my first visit with them if they wished an explanation of “How long do I have to live?” and “What will the process of dying be like?”. I recorded their responses in my visit notes.
The data demonstrated that 96% of the families were open to having these discussions.
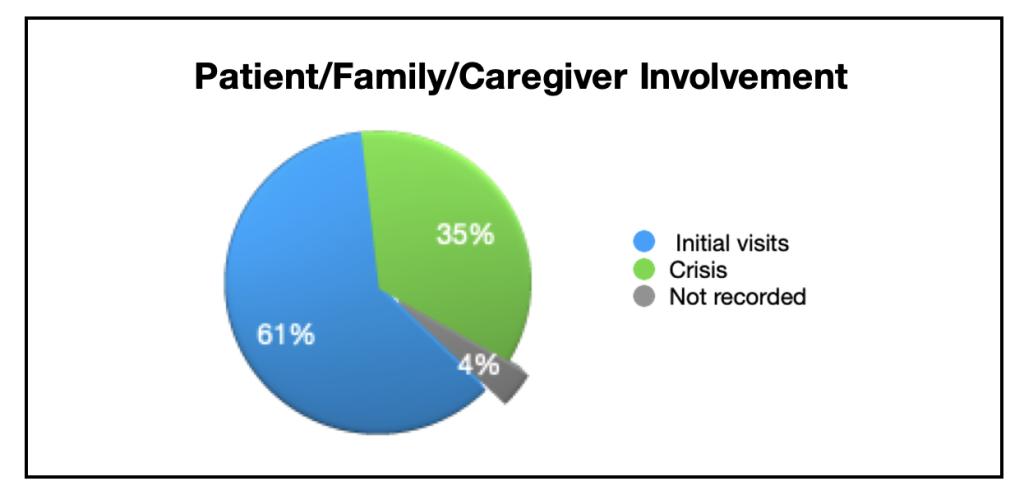
The chart depicted below demonstrates that 61% of the patients and families asked me the questions during my first visit. Another 35% requested explanations after we had successfully controlled a crisis together. The remaining 4% may or may not have wished to talk about these questions – no confirmation was recorded in my notes.
I felt it was significant that both patients and families wanted knowledge and participation in decision-making. This became a very positive factor in the success of my approach to the care. Year after year I became more convinced that families played the most important role in patients being able to remain at home for their care until death.
Although the data shows that 24% of the patients who died in the community required admission to a residential hospice in the final days of their journeys, the following graph demonstrate a more insightful explanation illustrating the number of days patients spent at home once they were referred to me for near-end-of-life care compared to the number of days patients spent in the residential hospice.
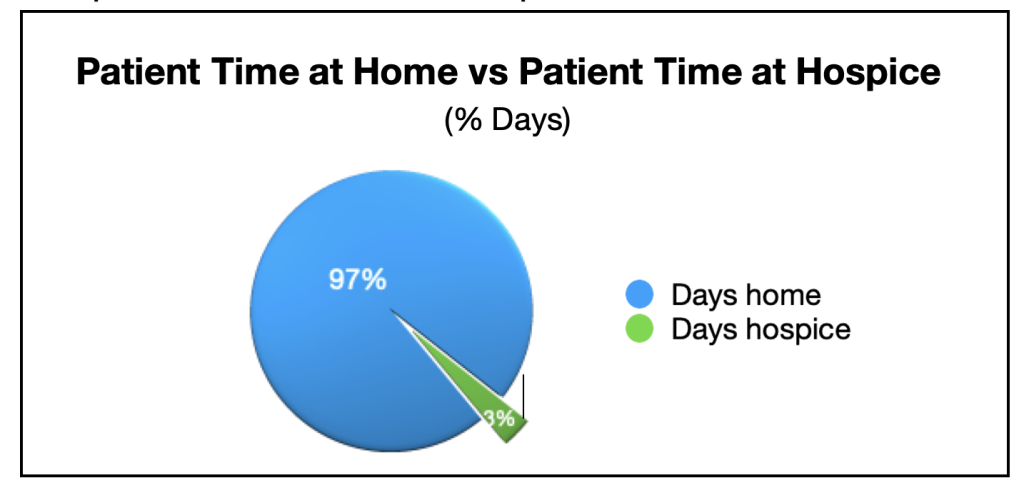
The pie chart clearly illustrates that most of the care was provided by families in their homes. Even though admission to a residential hospice, providing safety, physical care and emotional support was essential for 24% of the patients, the patients spent 97% of their near-end-of-life journey in their homes with the support of family. The admissions to the residential hospice measured a few days to a few weeks. The length of time families cared for their loved one at home with the help of community palliative care measured months to several years.
My general review confirmed that patients and families requested information, or were open to learning, about the science of the near-end-of-life journey. With this knowledge, families participated fully in the decisions of care, added their unique adaptations and art of the care throughout the journey and succeeded in their goal to care for their loved one in the community until death.