
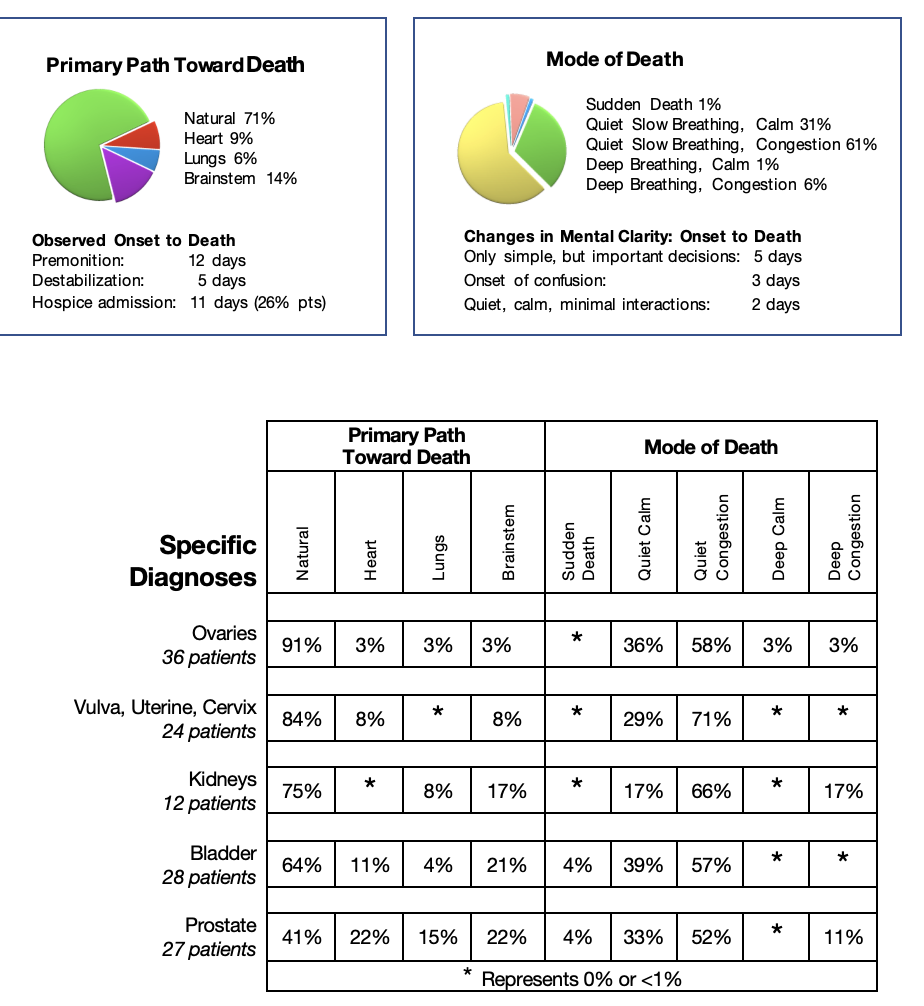
Patients with renal and pelvic tumours progressed mainly due to local abdominal spread causing bowel obstruction leading to liver failure, with the patients following the natural path toward death. If local disease was controlled by surgery or radiation, and stents cleared obstructed ureters, spread to lungs, heart, and brainstem was common leading to the erratic path toward death. The mode of death was usually quiet slowing of breathing often complicated by congestion from heart failure requiring Scopolamine to dry the secretions.
Kidney Cancer:
The most significant objective premonition observed in patients with cancers of the kidneys, indicating impending kidney failure, was the Kussmaul breathing pattern. It occurred more frequently than with the other cancers of this group. These patients followed the natural path toward death but with a more rapid deterioration.
Bladder Cancer:
The lower the location of the cancer in the pelvis, the less the digestive system was compromised. In patients with bladder cancer, the cancer often spread locally into the kidneys, but did so slowly, leaving enough normal tissue for the kidneys to continue their essential functions leading to the natural path toward death. If the cancer eroded locally within the bladder, it caused severe bleeding leading to the erratic path toward death triggered by heart failure. Over time, if the local spread did not interfere with the function of the essential organs, through blood flow, the cancer spread to the brainstem and lungs triggering the erratic path toward death.
Prostate Cancer: In patients with prostate cancer, the cancer tended to grow slowly within the prostate and remain asymptomatic for years. Once the cancer spread, it often blocked the rectum and the ureters. Resolution of the blockage with colostomies and nephrostomy tubes allowed the digestive tract and kidneys to continue their essential function, allowing time for the cancer to spread widely throughout the body, affecting brainstem, lungs, and heart triggering the erratic path toward death.
Specific Diagnosis: Ovarian Cancer
Natural Path Toward Death
Pre-referral Information:
Jeanne was diagnosed with ovarian cancer 19 years prior to her death. She presented with a pelvic mass, underwent an abdominal hysterectomy, removal of her ovaries, and half of her colon, followed by chemotherapy. Five years later, the pelvic mass recurred. It was treated by surgery to remove most of her tumour with no additional treatment, just follow-up assessments. Then six years later, she was admitted to the hospital with an upper respiratory infection, fever, and diarrhea. Investigations revealed ascites with scattered cancer lesions in the abdomen and pelvis. She was treated for her infection but refused chemotherapy. She remained well for another six years until she suddenly became very short of breath, had bouts of coughing, and weight loss. She was admitted to hospital, investigations revealing anemia, fluid around her right lung preventing its expansion, and multiple solid masses in all areas of her abdomen. She accepted a transfusion, was discharged home and agreed to a referral for community palliative care.
Initial Contact:
I first met Jeanne with her husband and adult children. It was now 17 years since Jeanne had been diagnosed with ovarian cancer. She lived through surgeries, chemotherapy and several hospital admissions revealing the ongoing, slow but relentless progression of her cancer. Jeanne and all in her family understood what was happening and that she would eventually die from this cancer. Presently her main issues were increasing ascites causing discomfort, shortness of breath on activity, bouts of diarrhea and fatigue. Jeanne sat through the interview, participating fully in the conversation and decisions. Her pulse was 84 and oxygen saturation was 88%. She stated she could perform her essential daily activities independently but very slowly, using a walker to ambulate. Her days were enjoyable with visits from her family, reading and going out to bingo weekly with her daughters. Her only medication was Metoprolol to control an irregular heart rate, diagnosed years before.
We discussed the approach to her care. She was very clear as to interventions she was prepared to accept. She did NOT wish supplemental oxygen regularly, but she agreed to have the oxygen in her home just in case of future needs. She did NOT wish pain medications nor drainage of the ascites. She DID wish regular visits for near-end-of-life care at home until her death. Jeanne remained amazingly stable for the next year. We made small changes to her diet opting for a low-fat diet with lactose-free milk. She ate well, with no nausea and no diarrhea. Her activity level remained the same including small household chores and her personal care. She had pain only over her left ribs but no need for medications.
Her pulse at rest remained around 63 and her oxygen saturation remained 98% without the need for supplemental oxygen. The abdominal bloating stayed much the same causing minimal discomfort. I continued to follow her every few weeks with a phone call and visited whenever she requested.
On-going Observations/Symptom Control:
One year before her death, we saw evident clues of Jeanne’s disease progression, becoming more severe every few months. Her world became smaller needing help to transfer due to weak legs. Her coughing worsened with her swollen legs as her abdomen became more bloated. Still, her vital signs remained normal. Every few weeks, we discussed issues to stabilize her functional ability, as well as prepare for the future. I explained various approaches to her symptoms, but she wished to continue our current treatment. During one visit she reported severe bouts of coughing especially early in the night. I knew she had cough syrup (a weak form of Morphine) in her home. I advised her to take a dose at bedtime for a week. To my surprise, she agreed, and found it beneficial!
Fusion of the Science and Art of Near-End-of-Life Care:
After we settled her cough, I took the opportunity to rediscuss the progression of her illness, the symptoms that might occur, the place of care when she could no longer transfer out of bed and the resources that would be available to her if she wished to remain at home. Again, Jeanne was very clear, “I am not afraid of dying. I wish to die at home.” We did not make any further changes in her medications. I simply advised her to reduce her fluid intake, using ice chips instead of glasses of water to reduce the swelling in her abdomen and her legs.
A few months later, Jeanne admitted to more fatigue. She could barely do household chores, limited by fatigue and shortness of breath. She did manage to go to bingo every two weeks. She looked well sitting, though pale, without signs of breathlessness. Her pulse was 80 and her oxygen saturation was 88%. She was thinking clearly. I asked Jeanne if her family and I could make practical changes to improve her ability to do her important activities during the day. She agreed. We reordered her supplemental oxygen in case of need. Her family, knowing how important her trips to the bingo were, set up a stairlift in the home and rented a wheelchair for her weekly bingo trip. I left an oximeter with Jeanne. She ‘loved’ the control it gave her. She agreed to the oxygen whenever the oxygen saturation was lower than 90% and during her trips to bingo. Jeanne was no longer afraid of taking her cough medication. She used it sparingly, but very effectively. With these simple changes, Jeanne did remarkedly well. Her ‘world’ settled; her bingo outings became enjoyable once more. She stabilized enough to enjoy a scenic boat trip on the St. Lawrence Seaway without exacerbating any of her symptoms.
Premonition:
Two weeks before her death, premonitions indicated Jeanne would soon destabilize. Jeanne reported, though eating well, she was experiencing diarrhea. She had removed all dairy products from her diet, but in the last week had at least three bouts of diarrhea through the night. Her leg swelling was much less, an ominous sign the diarrhea was having a marked effect on her hydration. Still, her pulse and oxygenation were normal. She was comfortable, so we made no changes to her medications. But on review of her diet, I discovered that she was still taking dairy products. We made new changes to her diet, hoping that her diarrhea would lessen, and she would be more comfortable.
Destabilization:
Three days before Jeanne’s death, her family observed more severe objective signs of destabilization. I was called urgently to visit. Jeanne had had severe nausea all night and in the early morning, she vomited a large amount. She had no diarrhea, no fever, and no pain. During my visit, she appeared very pale and anxious. Her oxygen saturation was 79%, improving to 97% with supplemental oxygen with a pulse of 105. Her abdomen was unchanged. Still, she was thinking clearly and stated, “I think I am about to die.” We discussed that, yes, she was weaker, but with bed rest, clear fluids for the next few days, she had a chance to resolve the diarrhea. She agreed to an injection of Gravol and ongoing Gravol tablets as needed and to all care in bed.
Two days before her death, during my visit, Jeanne’s family reported that she had no nausea or vomiting or diarrhea since my last visit. She had a good night without abdominal pain, but she needed her oxygen continuously, and today, she had slept most of the day. On the supplemental oxygen, in bed her vital signs were normal. The short time she was awake, her thinking was clear, and she asked for Jell-O. Her family was convinced she was starting to rally as she had done many times before. I was pleased that she was more comfortable, but I felt that her death was imminent within a few days.
One day before her death, I was contacted by Jeanne’s husband who reported that she had developed severe lower abdominal pain after passing a large amount of liquid stool. I advised a dose of her Morphine cough liquid as a pain medication and return to clear fluids only. When I visited in the afternoon, Jeanne’s pain was better, but she was much weaker and drinking just a little fluid. Still, she tried to transfer to the bathroom to void. She fell but did not injure herself. Jeanne’s family was very worried, asking, “What is happening?” Jeanne had survived for so long with minimal symptoms. In the last two weeks, it was evident that her reserve energy was exhausted, that her digestive system was no longer able to function for her needs. Still, the family saw that she was thinking clearly, appeared comfortable, so, “How could she be dying so quickly?”
As her family gathered, I explained again the significance of changes. Jeanne could no longer transfer out of bed, she could only drink a little clear fluid, she was sleeping most of the time and she was dependent on her supplemental oxygen. I reminded them that Jeanne had had an irregular heart rate for years, so her heart also had limited reserve. I explained that considering all the evidence we were observing, Jeanne would likely die in the next hours to a few days. I advised them to keep her in bed, giving her clear fluids only if she requested. I suggested that her family should keep a vigil at her bedside.
Jeanne had a quiet night, with her daughter sleeping at foot of the bed. When her daughter awakened in the early morning, Jeanne changed, became very still, and ceased to breathe within a few minutes.
Timeline to Death
Predicted: 1-2 months Actual: 24 months
Jeanne’s journey at near-end-of-life demonstrates a common progression of patients diagnosed with ovarian cancer, although her journey was much longer than most other patients.
Jeanne remained in control, thinking clearly, and making her own decisions throughout her near-end-life journey. She was not afraid of dying. She was happy with the little pleasures of her day-to-day routine and the support of her family.
She knew and told her family and I that she was close to dying three days before her death. Her family could not believe this reality, but they listened to her, remained with her, caring for her until she died three days later.