
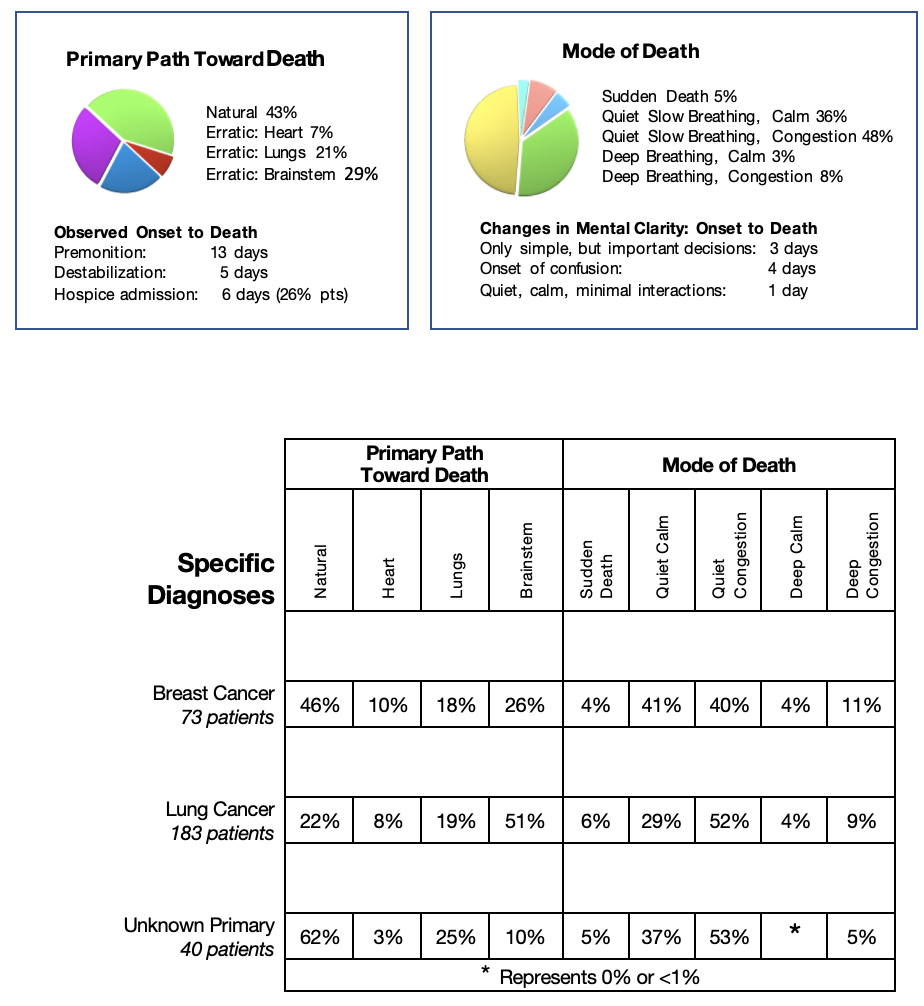
I was surprised to discover that breast, lungs and unknown primary cancers were so similar in their progression. On reflecting, I understood some of the reasons. The anatomical location of the breasts is just over the lungs and therefore local spread can quickly involve the lungs. Both breast and lung cancers are in areas of the body that lead to early diagnosis and treatment by surgery and radiation. The lungs, being essential organs for survival, have a great reserve and large blood vessels with access to all the essential organs in the body. With local disease controlled, widespread metastases from the breast and lung cancers are common to the liver leading to the natural path toward death, and to the lungs, heart, and brainstem, each site triggering the erratic path toward death. Between 25 – 50% of patients died from metastases to the brainstem. A plausible explanation is that the lungs with their large area and great reserve can tolerate more cancer deposits than the brainstem housed in a tiny area covered by non-flexible bone.
Unknown Primary Cancers
Patients with unknown primary diagnoses mainly followed the natural path toward death. I believe most of these cancers originated deep within the abdomen or pelvis with minimal symptoms early in their disease, making early diagnosis challenging to. By the time these cancers caused symptoms they had already spread widely, invading the liver, the closest essential organ most severely.
Significant Symptoms
Specific Diagnosis: Lung Cancer, Brain Metastases
Erratic Path Toward Death Brainstem Trigger
Pre-referral Information:
When Serge was referred to my community practice, the referral documents stated he had been diagnosed with cancer of the lungs, widely spread. His physicians predicted that he had two to six weeks to live. He fooled everyone and lived his life his way for eighteen months.
Serge, according to his wife, Dianne, was a man with the “eagerness to explore the world.” Both Serge and his wife started their careers as physiotherapists.
Both made significant changes throughout their lives together. Serge built his own computer consulting company and became very involved in the Ottawa community as a board member of the Children’s Hospital of Eastern Ontario (CHEO).
“It is not the number of days you have left in your life.
It is the life you have left in your days”.
Serge’s blog
Serge was diagnosed with lung cancer at 48 years of age when his daughter was a young teenager. He underwent aggressive treatment and did well for three years. He faced life as he had always done through those years, making every minute count. He also created a blog to help others living through the same experience. His cancer recurred, spreading extensively to his bones and brain, both the brainstem and the cerebellar areas. He underwent radiation to both areas understanding that the goal was not for cure but to improve his symptoms. He was told there would be no possibility of further active treatment, and his prognosis would be six weeks at the most. He agreed to a community palliative care referral.
Initial Contact:
I first met with Serge and his wife in their home. Serge participated in the conversation and understood his illness, but he allowed his wife to give the details. She reported that Serge was up and about, still going out of the home every few days always accompanied. His main symptoms were general weakness, unsteady gait, and changes in his mentation. The changes were subtle and complex to discern clearly due to his concurrent hearing loss. His wife observed that his mind processed complex issues more slowly. He had difficulty with calculations. He had been an avid reader and read several newspapers daily. Now he had little stamina for reading. He had expertise with computers. Now he could no longer use the computer. Serge had “episodes” of frequent headaches and dizzy, lightheaded spells. They occurred suddenly, especially when he was tired and cleared spontaneously with rest. As Serge had been all his life, he was reluctant to take adequate medication for the headaches. He did agree to a small pain patch changed every three days for back pain. He had Hydromorphone tablets to take as a breakthrough but rarely used them. To prevent side effects of increased intracranial pressure during the radiation to his brain, he was started on Decadron tablets four times each day. The plan was to taper the dose when he stabilized.
Both Serge and his wife had the same goal – the best quality of life possible with all the care at home. They both understood that the prognosis would likely be very short.
Serge, however, was quite distant, not very talkative through the interview as if his thoughts were far away. Through Dianne, I clearly understood that Serge wanted better control of his back pain without negatively impacting wakefulness, functional ability, and mentation. Dianne was realistic and wanted education about Serge’s illness: “What are these episodes of headaches and dizziness? Are they an indication of a life-threatening event? What is likely to happen as Serge’s disease progresses? What are the resources that will be available to me in the care of my husband at home?” Serge and Dianne were part of a very loving and supportive family. Many members of the extended family were in town and ready to help. Their daughter, Emilie, was in high school, doing very well. She understood the seriousness of her father’s illness and was part of the discussions regarding his health. Serge’s wife, Dianne, had kept herself well informed. She was committed to Serge’s care. I had no doubt the family would care for Serge at home.
I too was apprehensive about these episodes. Serge had had a very active life. Intellectually, he had been highly functioning. From our discussion, I observed that he had difficulty with simple tasks and could not engage fully during my first visit. I felt these ‘episodes’ might be an ominous indicator of increased intracranial pressure, seizures or minor strokes, not well controlled even with very high doses of the steroid, Decadron. I felt the prognosis might be very short. I was worried enough to quickly order injectable medications brought into the home to prepare for any crisis. Still, his vital signs were normal, so I felt we had a little time to assess. I also wanted Serge’s pain to be better controlled while keeping the regime as simple as possible.
On-going Observations:
Dianne and I were very close in our thinking and approach to Serge’s care. We both felt it would be good to prioritize the pain issues in the first few visits. Visiting frequently would allow me to monitor Serge’s ‘episodes,’ which were much more worrisome than his back pain. Over the first two visits, we made minor adjustments to Serge’s pain medication. We changed his patch regime to every two days. I asked Serge to take the Hydromorphone tablet regularly on awakening and at bedtime and whenever his back pain or headaches started. I explained that this regime would not increase his fogginess, but he would rest better and move about more easily. It was evident within a few days that this regime was very beneficial. His wife reported that his ‘episodes’ were less frequent and less severe. She could quickly discern the early signs and pace his activities with good effect. His pain was better controlled.
Premonition: Serge’s episodes
Over the next month, Serge appeared to be recovering from the radiation side effects and reaping the benefits with improved mentation in the day and better sleep at night.
Still, during the day, he required more breakthrough Hydromorphone for sharp, low back pain occurring with activity. The unexplained ‘episodes’ were becoming more frequent again, increasing in severity and lasting longer. They were still triggered suddenly by activity and evolved to include neck pain. They still resolved spontaneously with rest. In the hope that they were atypical seizures, we started a small dose of the tranquillizer/ anticonvulsant, Clobazam, at bedtime to minimize any sedation during the day. We also asked Serge to decrease his excursions outside the home for a few days, and we monitored him carefully.
He did not improve and was more tired and weaker on transfers. Therefore, we stopped Clobazam to assess his condition for a few days without its effects. I visited his home the day after Clobazam was stopped. Serge was his usual self, though more tired. Then suddenly and very dramatically, we observed an “episode.” He suddenly had a marked change in his cognitive ability, no longer responding to directions, unable to speak. We were just able to direct him to the sofa quickly and lay him down. He then developed a profound Cheyne Stokes breathing pattern. His oxygen saturation plummeted down to the low 80s, his pulse up over 120. There was no congestion. At times he seemed to be very uncomfortable holding onto his head. The appearance was one of a sudden massive increase in intracranial pressure or possibly an atypical seizure – both seemed life-threatening. The goal was to keep Serge at home. When I asked Dianne, during this severe crisis, if this was still goal, she confirmed that Serge would stay home.
Symptom Control:
Our first task was to stabilize the symptoms and regain comfort quickly. For pain, I doubled his patch and administered Hydromorphone, twice his usual dose, subcutaneously. Because he could not swallow, I changed his usual oral Decadron to a double dose subcutaneously to stabilize his intracranial pressure. In case the symptoms we were observing were due to an atypical seizure, I administered an intramuscular injection of the anticonvulsant Phenobarbital. Within a half-hour, he seemed much more settled, his oxygen saturation improved to the low 90s, and his breathing was less laboured. We decided to set up nursing shifts for the evening and night to monitor and administer injectable medications if the episode recurred or progressed further. I ordered oxygen by nasal prongs urgently for comfort.
I explained my assessment to his wife indicating that I was preparing for the worst outcome but still hoping for the best with some recovery. We agreed to follow up with a phone call to determine if I needed to visit in the evening. His prognosis had been 2-6 weeks – it was now over four weeks – his wife understood the gravity of the symptoms.
Rebalancing/Stabilization:
When I called in the evening, Serge had remained settled and comfortable, awakening on and off for a few minutes, eyes opening, focusing a little and able to say a few appropriate sentences, reporting he no longer had a headache. His breathing returned to a normal pattern on supplemental oxygen. The nurses were in place. We decided to continue injectable medications for the night, Phenobarbital and Decadron at bedtime and Hydromorphone every two hours as needed for headaches and laboured breathing. I visited the following morning, hoping for an improvement in Serge’s condition. When I arrived, everyone was excited, reporting Serge had passed a good night and was now considerably improved. His breathing was essentially normal, with oxygen saturation 88% on room air and 92% on oxygen. He denied any shortness of breath. His headaches were gone. He tolerated the increase in the pain patch without side effects and did not require any breakthrough Hydromorphone through the night.
Within 24 hours, Serge was back again! His mentation was much clearer, his appetite returned. Over the next few days, he stayed upstairs and had frequent naps in the day, but he was comfortable, had much less back pain, and started to increase his activity. To our further amazement, his functional ability and mentation were much improved. He was now better than he had been since his radiation. He was able to walk to the bathroom to shave. He discussed what had happened the last few days and what might happen again in the next few days. He was hungry, requesting to eat as soon as possible. And he was eager to start regular activities. We convinced him to do so in his bedroom for the day.
His wife and the nurses reported that Serge could not be held back the next day. He had had no further episodes; he continued to think more clearly than he had in weeks, ate well, had no headaches and no need for extra medication for pain. Before my visit, he did his care, then walked downstairs with good balance, no shortness of breath without oxygen to greet me, looking very pleased with himself. His oxygen saturation on room air was 96%; his pulse was 96 on activity and 77 at rest. He was back!
He improved still further over the next few days, though a little more slowly. He tolerated a shower with help but realized he needed to rest for a few hours after the effort. He slept longer in the morning but awoke with a clear mind. He did not have any episodes, just an occasional minor headache requiring no extra medications. Slowly he started to increase his activity. He managed the stairs; he walked about his home and into his garden. We continued his regular medications, but now the Decadron, Hydromorphone and Phenobarb were tolerated orally. His patch remained at the higher dose.
We all agreed that if he had a recurrence of his severe episode, we would return to the same injectable regime as before.
There was no recurrence over the next few weeks. Serge continued to improve both in mental clarity and physical stamina. He was able to go out daily in the car. His walking balance and energy were much better, only limited by increasing low back pain. He had occasional tightness in his head, not severe enough to take medications. He could make some lists, help plan his day, enjoy outings. He was sleeping reasonably well but with vivid dreams.
A New Premonition:
A few weeks later, Serge suffered a minor but apparent complex seizure. His oxygen saturations remained normal on room air, and his breathing did not change. We knew now that though he had greatly improved, he was very fragile! Serge had two problems limiting his activities and quality of life – atypical seizures and low back pain. Serge continued to be very clear that if he was going to live longer, he wanted to be active.
The first problem was the seizures. We had waited and monitored. They were recurring unpredictably, but usually with activity and therefore trips outside of the home had a high risk. On the other hand, increasing the Phenobarbital to a regular twice daily regime would likely make Serge too sleepy to do his desired activities. We compromised and increased his Phenobarbital by adding a half dose in the morning.
The second problem was the increasing severity of low back pain. A single dose of radiation might resolve the pain permanently, allowing him to increase his activity. The risk was that the stress of the treatment might destabilize his fragile body. We were at six weeks past his estimated prognosis. He was having seizures demonstrating that the disease in his brain was active. Serge was now mentally clear and participating in these discussions and decisions. It did not surprise us that he chose the radiation to be more active and to live in the time he had left. I explained to Serge that the back pain might increase due to an inflammatory response in the first few days after radiation. Therefore, to maximize the benefits of radiation and minimize the side effects, I asked Serge to take Hydromorphone immediately with any exacerbation of pain, at least for those few days.
Serge’s recovery from radiation was not easy. His wife and I wondered if he would ever regain his functional ability. He had the side effects expected from a large dose of radiation: increased back pain interfering with all his activities of daily living and marked increase in his fatigue. His large doses of Decadron would decrease the swelling from the radiation, so we hoped that within a week, both would resolve.
Serge agreed to Hydromorphone by injection at bedtime to help with comfortable sleep, allowing healing to occur more quickly. My greatest fear was that the stress on his body from the radiation would trigger his “episodes.” And yes, he did suffer more episodes, but they were minor, his vital signs and breathing patterns remaining normal throughout.
Ten days post-radiation, he still had not improved. He was more somnolent, and his wife had difficulty awakening him for meals. His thoughts were disjointed and difficult to understand. The good news was that he had no further major ‘episodes. I wondered if these changes were signs of increased intracranial pressure. Perhaps, he was not absorbing the oral Decadron well causing the intracranial pressure to rise. We had an easy and quick way to discern which theory was correct, by changing his usual dose of Decadron to twice a day given by injection. Within 24 hours, Serge was back again! His mentation was much clearer, his appetite returned. Over the next few days, he stayed upstairs and had frequent naps in the day, but he was comfortable, had much less back pain, and started to increase his activity.
Severe Episode:
One week later, another setback. Serge suffered a severe ‘episode.’ He suddenly developed a central breathing pattern; his oxygen saturation quickly decreased to 78%. He did not lose consciousness, had no pain, no seizure, no headache but some tightness of his chest. His wife applied oxygen. I advised giving Hydromorphone and Decadron subcutaneously quickly and then continue the extra dose of Decadron for the next few days. He continued to have a central breathing pattern overnight, but his oxygen saturations remained about 90%, and he slept comfortably until early morning. He then awakened fully alert, hungry for breakfast and trying to walk about his room. He soon realized he needed to pace his activities carefully. Still, over the next three days, he recovered his mentation and functional ability, slept well, had no seizures, ate well, and his pain was well controlled. By my next visit, he had managed the stairs and had a wheelchair tour of the garden. We all decided to continue the regular Decadron dose at breakfast and lunch and a half dose at supper.
And then Serge had seven months of stability! He reaped the benefits of the improved pain control and the control of his ‘episodes’ without any changes in his baseline medications. However, his wife and I knew the fragility of his situation. We knew the disease would continue to progress and that our symptom control regime was masking the underlying progression of Serge’s disease.
Fusion of the Science with the Art of Near-End-of-Life Care:
Based on our experiences with the sudden exacerbations of his episodes with stress, both physical or psychological, his wife and I devised a ‘rescue regime,’ a system to quickly control or abort the serious complications quickly whenever they occurred. We knew we had to have this plan in place because, true to Serge’s character, he was now going to get as much out of life as possible. Serge’s family, especially Dianne, had now learned to take back control with a clear understanding of the illness and medications and a realistic approach to Serge’s goals. Serge and Dianne were self-directed, accomplishing goals way beyond expectations, and helped by a secure and easily accessible medical link through me for advice.
Dianne carried her “rescue kit” with her for any trips out of town. She was the expert on Serge’s behaviour, monitoring all Serge’s activities. She knew the early signs of an impending ‘episode.’ She would insist on immediate bed rest and clear fluids for up to twenty four hours. On an overnight trip, she brought a commode into the hotel room in case he could not walk to the bathroom. The rescue medications were prepared in three syringes for subcutaneous injections, one syringe each of Decadron, Hydromorphone and Phenobarbital to be given according to the severity of the episode. She had a telephone link to me for advice and support. I would visit the day before and after a trip to assess and advise.
And Serge just started to do what he did best. He made plans to do things and live life to the fullest. First, he increased activities in his home by managing the stairs independently, reorganizing his basement workshop, working on the computer to set up his family photo album and reading several newspapers every day. Then, he extended his activities outside his home. He cleared out his work office and went out with his wife most afternoons just for the excursion. Serge decided he was well enough to continue to serve on the board at CHEO, he helped organize his anniversary celebration at the Chateau Laurier and enjoyed the dinner with his family.
Serge continued to tolerate all these activities well, so he decided to attend events out of town. His wife and I were skeptical, but we were proven wrong! He attended a Children’s Hospital board meeting in Montreal without incident, well enough to give the summation speech. He set up and enjoyed several weekend trips to resorts outside of Ottawa with his daughter and wife. As Christmas approached, Serge up the Christmas lights around his home, constructed the family Christmas village on the mantle and went to the Christmas celebration at his sister’s home. And since he felt he was not dying, of course, it was essential to have his teeth cleaned and his regular yearly eye examination.
Ominous Premonitions:
In late winter, Dianne and I started to see some significant changes. He was not sleeping as well. He had achiness and swelling of his legs, weakness of his quads, facial swelling – all side effects of long-term high dose Decadron. But, from Serge’s perspective, he had been feeling so well that he began to question if he had cancer in his brain. His wife, monitoring Serge closely through all the activities, knew how fragile he was. She predicted and prevented any severe episodes and paced his activities so well that Serge was oblivious to his fragility. I knew the only way to reduce the steroid side effects was to wean off the Decadron. But I knew that any decrease in the baseline Decadron would quickly destabilize him.
Already he was having great difficulty with the stairs, due to weakness in his legs and imbalance from his brain metastases. Even after many attempts to persuade him to set up all his activities on the main level, he refused because he wanted to continue to sleep with his wife upstairs in their bed. Although Serge was more limited physically, his mentation remained reasonably stable. He was able to play scrabble with his sister, translate moderately complex scientific language from English to French and enjoy the company of his friends and family. Our concerns with the stairs were settled when he tore his Achilles tendon one spring day while climbing up the stairs. Walking and transferring were challenging, but stairs were impossible.
Fusion of the Science with the Art of Near-End-of-Life Care:
A family discussion ensued as to what to do. To minimize the progression of the disease as predicted by the premonitions we needed to preserve Serge’s energy. Serge wanted to pay for a stairlift to continue to sleep upstairs with his wife. Instead, his family suggested using the money to find ways to continue to be outdoors during the spring and summer. And to everyone’s surprise, Serge relented. The family mobilized! They rented a scooter allowing Serge to drive along his neighbourhood streets talking to his friends and work in his garden (with Dianne running after him to prevent an accident). For Serge’s birthday, his wife bought him a hot tub. Dianne, being a physiotherapist, with the help of his family, found a way to transfer Serge from bed to wheelchair to hot tub using ramps and a mechanical lift. Whenever Serge was in the hot tub, the emotion written on his face was one of sheer rapture! His family set up a hospital bed and a bed for his wife side by side in the living room on the main floor so Serge could sleep with her, and his daughter could spend quiet evenings with her father and mother watching TV or just quietly talking. We set up nursing shifts for the personal care in the day to give respite to his wife and convinced Serge to have most of his personal care in bed to preserve energy for ‘fun’ activities.
With these adaptations, Serge had another few months of stability. Then signs of progression increased, as demonstrated, not with ‘episodes’ but with increased pain on activity, pulse rate over 110 even at rest and an agitated confusion leading to poor sleep in the night. He was still active, now limited to using the scooter or the hot tub only every few days. We increased his pain patch slightly and started a small dose of Nozinan at bedtime regularly. Occasionally, we needed to use his ‘episode’ medications in the night to help with his sleep. And again, he settled remaining stable for another month.
Destabilization:
One month before his death, Serge’s world became his bed. This was a clear premonition that he would soon destabilize. His wakeful time was mainly in the evening, spent with his wife and daughter quietly watching TV or just being together. We converted all his medications to subcutaneous injections. We increased the doses slightly to better control his symptoms while allowing him to have lucid moments during the day and evenings to interact with his family and eat and drink as he tolerated. He was less active, so he did not trigger his back pain. And in the last few days, we needed to increase his Phenobarbital to a regular dose twice daily to control more frequent short seizures. Discussions turned to concerns for his daughter. A referral was made to a social worker to provide her with bereavement counselling. His wife kept the school staff updated with Serge’s changes. We ensured that Emilie was present during my visits to participate and ask questions about her father’s progression and imminence of death.
Up to a few days before his death, Serge still had short wakeful periods in the evening when he could interact with his family.
Death Imminent:
One day before his death, Serge slept comfortably. Many family members visited, and though he did not speak in sentences, he could make short appropriate responses to each. During my visit, I observed evidence of destabilization. He was congested, had a rapid steady central breathing pattern, oxygen saturation 80% on oxygen and a pulse of over 130. I explained the changes to the family and started regular Scopolamine, Hydromorphone and Nozinan every four hours for comfort. In the evening, I called his wife. He was very calm and comfortable, but his vital signs continued to deteriorate through the evening for the first time in his illness. This was ominous! Serge had always been better in the evenings. I explained to his wife that pressure in the brain usually increased during the night and that I felt Serge would not live beyond the night. Serge slept quietly through the night with his wife beside him. He slowly weakened, breathing with less effort, and died peacefully in the early morning hours with his wife beside him.
Timeline to Death
Predicted: 2-6 weeks Actual: 18 months
Serge used the time given to him exceedingly well remaining true to his goals in life – to live his life to the fullest. It was not easy to maintain the equilibrium between comfort and activity, but thanks to his wife and extended family, we could do so for him way beyond our expectations. Each excursion beyond his home and especially out of town, enjoyed by Serge, brought him to the edge of death. His wife recognized that fact. She was realistic and observant and managed to organize the events, despite her fears, to maximize Serge’s enjoyment and rein him in with rest and medications to prevent the inevitable crisis such an expenditure of energy would cause.
Serge’s daughter Emilie was the greatest beneficiary. She was able to continue to see Serge as her father, adhering to his philosophy of life despite facing his death. She was able to participate in his journey right to the end. All involved in Serge’s care were amazed that Emilie could speak at her father’s funeral. One of her school assignments had been an essay entitled “A perfect day in my life.” She chose a day during a holiday in England with her father and mother. In that essay, she captured the essence of her father’s life – Serge’s ‘eagerness to explore the world and live his life to the fullest’.