
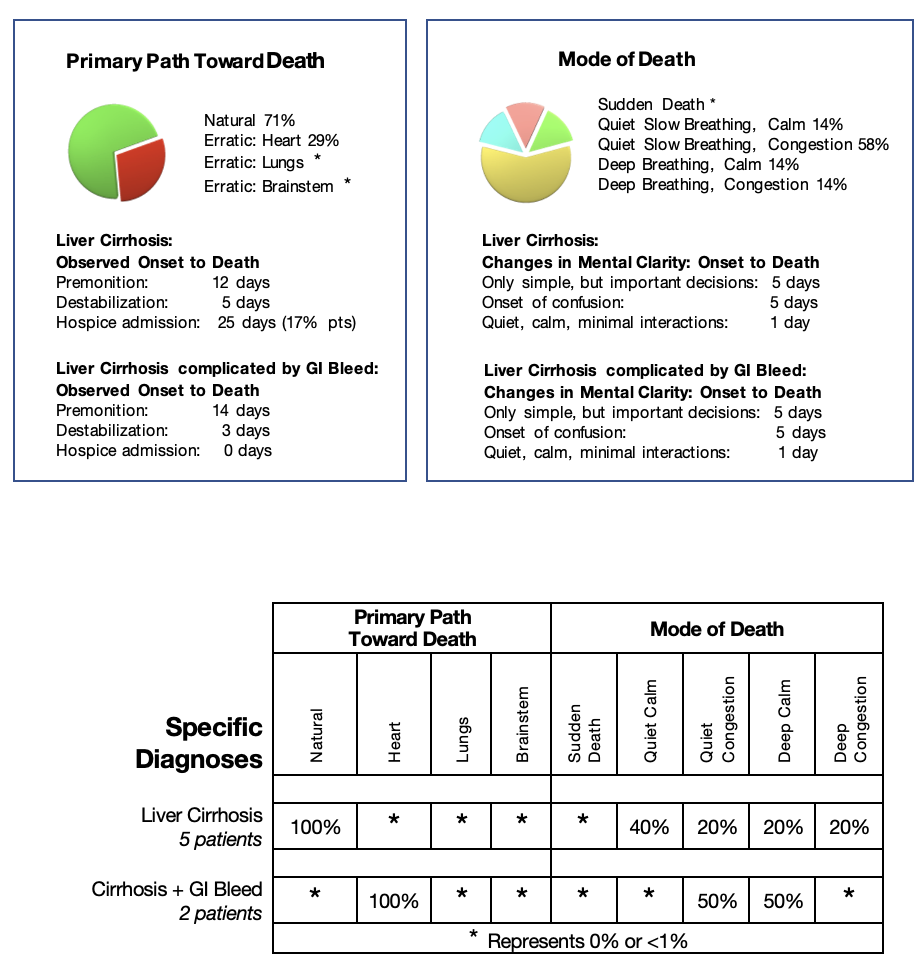
All my patients diagnosed with liver disease causing cirrhosis led to liver failure. They usually had a very long early history of increasing compromise of their liver, but due to the vast reserve of the liver, they remained asymptomatic and did not come to medical attention until they developed jaundice or gastrointestinal bleeding. Of these patients, 75% eventually could no longer process food for their body’s needs as cirrhosis scarred more and more of their liver. They followed the body’s natural path toward death as expected. The remaining 25% followed the body’s erratic path toward death triggered by heart failure. As the scarring from the cirrhosis extended, it encircled the blood vessels bringing nutrients to the liver, compressing their walls. Blood could no longer flow optimally into the liver. Instead, the blood backed up into vessels of the esophagus and stomach, stretching and rupturing their walls causing massive gastrointestinal tract bleeding and death from heart failure.
Specific Diagnosis: Non-Alcoholic Hepatitis
Natural Path Toward Death
Pre-referral Information:
Gerard, 83 years old, was referred to community palliative care with the diagnosis of non-alcoholic cirrhosis after a tumultuous six months of uncontrolled symptoms despite many investigations. He had presented with ascites, a fatty liver, an enlarged spleen and blood work indicating liver dysfunction. He was presumed to have alcoholic cirrhosis, though he denied drinking alcohol. His previous history complicated the search for a definitive diagnosis. He had been diagnosed with chronic kidney failure, non-life threatening, a few years before. His ultrasound demonstrating the fatty liver, also identified a partial blockage of his ureter from a kidney stone. He also had sleep apnea requiring a mask at night to assist his breathing, hypertension, depression, and chronic anemia. His kidney stone was removed stabilizing his kidney function. There was no treatment given for his liver problems. Three months later, he was readmitted with increasing confusion. A CT scan of his brain revealed only age-appropriate changes. His blood demonstrated elevated ammonia levels, consistent with increasing liver disease causing confusion. He was treated with Lactulose and sent home. One month later, he was readmitted with shortness of breath, confusion, and generalized weakness. The cardiologists found no significant problems. The gastroenterologists diagnosed non-alcohol-related cirrhosis, treated him with diuretics, and made a referral for community palliative care.
Initial Contact: Two weeks before his death, I visited with Gerard and his son. Gerard was in bed but alert, oriented and fully participated in the conversation and decisions. We reviewed the tumultuous history of the last six months. He was very frustrated that no one had believed he was NOT an alcoholic in those six months.
The high dose of Lactulose, prescribed while still in the hospital to lower his ammonia level and help with his confusion, caused severe diarrhea, so Gerard stopped taking it. Now his bowels were working well, and he was eating much better with no nausea. Gerard had no pain. He coughed when transferring from bed to bathroom, but it settled with rest. On the diuretics, he had lost over sixty pounds of fluid decreasing his abdominal girth and the swelling of his legs. He looked well and was able to sit up with some help. Gerard’s pulse was 59, oxygen saturation was 96% without supplemental oxygen with a low blood pressure at 88/40. His abdomen was soft, with a palpable mass – either an enlarged liver or spleen. He had minimal swelling in his lower legs. Gerard stated that his main issue was, “I cannot sleep at night. I cannot tolerate my CPAP mask.”
I felt that Gerard’s liver cirrhosis had stabilized since his return home, probably because he was well cared for by his son. Still, he was fragile and would need careful monitoring. Together we simplified his medications, continuing only his diuretics and his sleeping pill, Trazodone. I tried to respond to the problem he perceived to be the most important. I agreed that he needed to sleep better at night. Therefore, we decided to try a small dose of Lorazepam at bedtime, added to his sleeping pill, and reassess his symptoms weekly.
Premonition:
One week before his death, I visited with Gerard and his friend. His friend reported that Gerard had been lucid since my last visit but more tired. His appetite was good, with no diarrhea. Gerard’s sleep was still poor, though taking Lorazepam nightly. His blood pressure was back to an acceptable level and oxygen saturation was 94%. I doubled his Lorazepam at night. Gerard’s son called the next day to report that his father had tried to get up by himself and fallen three times in the last 24 hours. His son was desperate, not knowing if he could continue his care at home. We set up all care in bed for the next few days using a urinal and diaper for his urination and bowels and scheduled a visit in two days to reassess his symptoms and discuss the place of care.
Five days before his death, Gerard had deteriorated further, too weak to transfer out of bed. The positive observations included sleeping well at night with no further danger of falls and normal vital signs. Gerard did have new problems including, difficulty voiding causing distress, and very slow, but appropriate mentation. In our discussions, his son realized that his father would die soon. I, too, felt that Gerard was about to destabilize. I explained the science of the changes. Gerard’s liver could no longer digest food, so he was weaker and weaker. His liver could no longer remove waste products, leading to his confusion.
Gerard’s son decided to care for his father at home, requesting some extra help. To help Gerard continue to sleep well, we stopped his diuretics and added Nozinan to bedtime Lorazepam and a urinary catheter. We set up shift nursing, and injection equipment to administer medications when Gerard could no longer swallow.
Destabilization:
Three days before his death, Gerard was still restless and confused in the night despite the changes we had made. He had started to choke while drinking. His breathing changed to a Kussmaul breathing pattern with no congestion. His vital signs remained normal. Gerard responded minimally during my visit. We stopped all the oral medications and started Nozinan one vial every four hours regularly and a half vial of Midazolam as needed, both subcutaneously. If Gerard continued to be confused at night or if congestion developed, we had Phenobarbital and Scopolamine available in the home.
Two days before his death, after a difficult night with moderate agitation, in the morning Gerard settled with the combination of Midazolam and Nozinan. During my visit, Gerard was sleeping comfortably with only slight agitated movements. His vital signs remained unchanged with the same Kussmaul breathing pattern. We continued the Nozinan and Midazolam every four hours and added Phenobarbital one vial twice daily regularly.
Death Imminent:
One day before his death Gerard was comfortable on the new regime. Still, he continued to deteriorate with congestion in his throat. When coughing, his lungs were clear, but his oxygen saturation decreased to 70% with a weak pulse. His lungs were clear. Scopolamine was available to the nurse if the congestion progressed. I explained the changes to his son, who realized his father’s death was imminent. Gerard’s son called me the following morning to report that his father had ceased to breathe quietly while he sat beside him.
Gerard’s story demonstrated the difficulties of diagnosing older patients with non-cancer diagnoses. Usually, they have multiple illnesses, non-life-threatening, but all potentially reduce the essential organ’s reserve energy. All these vital organs could be the trigger for sudden deterioration.
In Gerard’s case, he had documented chronic ‘kidney’ failure as well as chronic anemia, hypertension, and swelling of his legs signifying ‘heart’ dysfunction. He had sleep apnea requiring external breathing support at night signifying ‘lung’ or ‘brainstem’ dysfunction.
His increasing confusion could have been a symptom of any of his underlying problems. But with his ammonia level so elevated and his ultrasound demonstrating an enlarged and cirrhotic liver, all the physicians quickly concluded that all the changes were alcohol damage to his liver. The problem was that Gerard did NOT drink alcohol.
Eventually, the gastroenterologist did believe him and diagnosed an autoimmune cause of his cirrhosis. His frustration of being ‘mislabeled’ as an alcoholic in the last six months of his life did not affect the treatment of his cirrhosis nor the length of his life. Still, it did affect the quality of his life, leading to six months of frustration with the medical experts rather than focusing on the quality of the limited time he had to live.