
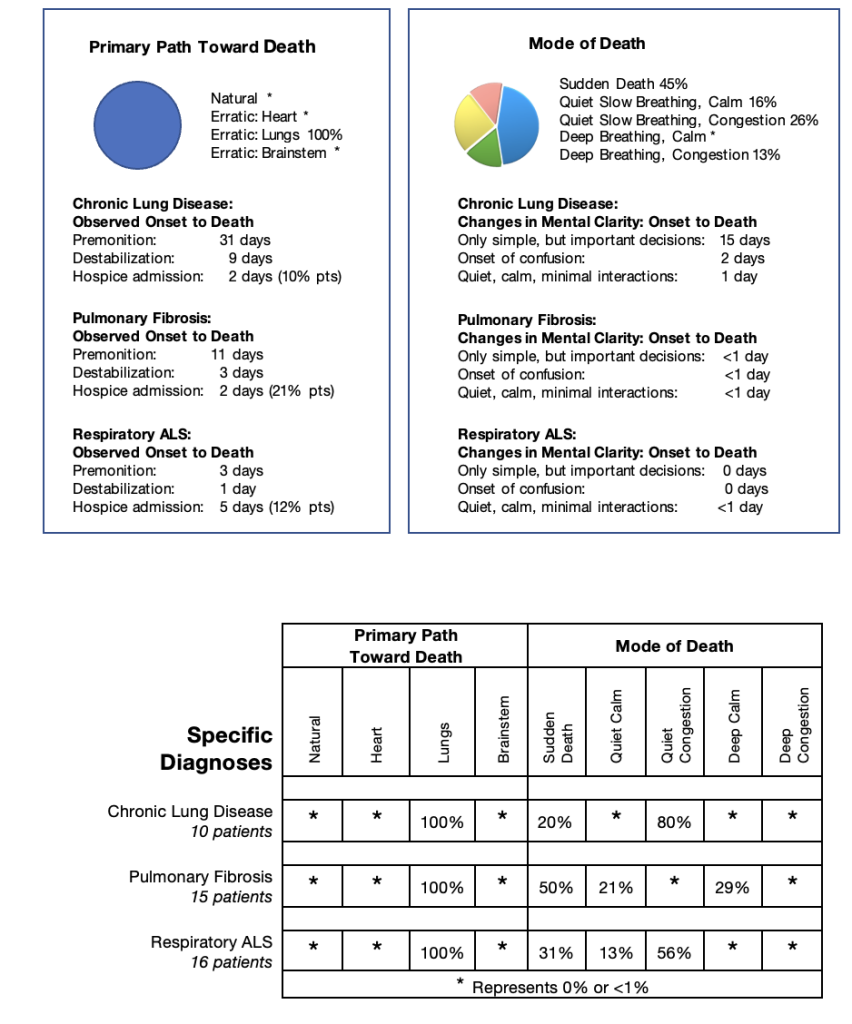
All the patients in my data set diagnosed with lung disease progressed through the body’s erratic path toward death triggered by lung failure. More patients died of sudden death than within any other group. The timeline from destabilization to death was very short and the symptoms very distressing. The need for regular Hydromorphone, Phenobarbital and Scopolamine averaged only one day. The need for regular Nozinan averaged two days.
My use of Midazolam was very different for patients within this subgroup. I found Midazolam useful very early in respiratory episodes causing severe shortness of breath during activities. In a number of patients, I started intermittent Midazolam over a year before death. The patient and family learned to predict which activities repeatedly caused shortness of breath and anxiety, administered a dose of Midazolam prior to that activity helping to maintain and enhance functional ability while preserving the patient’s clarity of thought due to the drug’s very short duration of action. Before my care, these patients had been given small doses of opioids for their shortness of breath triggering anxiety. These drugs were effective but not well tolerated because they tended to cause drowsiness from their longer duration of action, and constipation leading to exacerbation of shortness of breath trying to pass stool.
Each of specific diagnoses in this subgroup attacked the respiratory system in unique ways. Therefore, I reviewed them individually.
Chronic Obstructive Pulmonary Disease (COPD):
Patients with COPD present with damage of the bronchi, bronchioles and the structure of air sacs leading to mucus obstruction observed by coughing leading to infection, and constriction and spasm of the airways leading to shortness of breath. These symptoms are controlled with a variety of puffers, nebulizers, antibiotics, steroids and increasing reliance on supplemental oxygen. Acute episodes often require hospitalization.
Pulmonary Fibrosis:
Patients with pulmonary fibrosis present with a progressive attack of the lungs’ air sacs (alveoli). The alveoli have a very fragile covering that functions as a filter for the lungs to transfer oxygen into the bloodstream and carbon dioxide out of the body. This delicate tissue progressively becomes thickened and scarred, no longer allowing filtration of the air. The scarring process is slow but unrelenting, affecting more and more alveoli until oxygen transfer is no longer possible.
It is a restrictive pulmonary disease because the scarred alveoli can no longer expand. Early in the illness, low doses of steroids are helpful. As the lungs are more and more restricted supplemental oxygen requirements increase. Puffers and nebulizers are rarely effective, antibiotics are rarely needed, and patients rarely need hospitalization.
Respiratory ALS:
Patients with respiratory ALS present with a very different attack on the respiratory system. The disease does not cause ‘any’ disruption of the lung’s structure, airways, or alveoli. Still, it leads to a restrictive respiratory failure from factors outside of the lungs affecting the chest wall muscles. These muscles, essential for the expansion and compression of the lungs, become weaker and weaker and eventually, the lungs cannot bring oxygen into the air sacs or blow out carbon dioxide. In my data set, patients with respiratory ALS were introduced to external assistance of breathing with BiPAP in the early part of their disease, used mainly at night to learn to adapt to the machine. As the disease progressed, the BiPAP was needed longer and longer until it could not be removed without severe shortness of breath. Patients were seldom admitted to the hospital. Instead, they were usually assessed and equipped with aids to help reduce exertion as outpatients at an ALS clinic. Supplemental oxygen was rarely beneficial because once air entered the alveoli, the lungs functioned efficiently. Midazolam was very useful to calm the breathlessness with activity.
Patients with respiratory ALS felt normal at rest and on BiPAP as they progressed. They did not believe they were close to dying, often until the last few days, when the premonition evidence of low oxygen levels while on the BiPAP was observed. Destabilization and death occurred within only a few days. Therefore, it was very challenging to discuss near-end-of-life issues with patients and their families early in their journey toward death.
Specific Diagnosis: Chronic Lung Disease
Erratic Path Toward Death Lung Trigger
Pre-referral Information:
Madge, 80 years old, was first diagnosed with COPD twenty-four years previously, being followed by a respirologist throughout the course of her illness. Five years before her death, she was admitted to the hospital with a severe respiratory crisis, presenting with an oxygen saturation of 80%, severe anxiety, generalized weakness, and unsteadiness. She recovered but was told that there was no further active treatment possible, and she would likely have only a few months to live. It was at that point that she asked to be referred to community palliative care.
Initial Contact:
I first met Madge with her two sons at her home a few weeks after I received the non-urgent referral. She had continued to improve and was now walking independently while on a high flow rate of supplemental oxygen. Her mentation was clear. She led the interview stating the purpose of the visit was to build a relationship with me. She knew that she would die in the next few months and was preparing her care to ensure she could remain at home until her death.
We reviewed her activities on a typical day. She stated, “I awaken early, read the newspaper in bed. Then I go down to the basement where I have all my crafts, a TV, and a bathroom and stay most of the day until bedtime. I live with my son, who does the groceries, cooks my meals, bringing them to me usually in the basement. I have three dogs which I love dearly. My son helps me care for them. I love them dearly. Occasionally I go out to craft stores to buy my supplies. But each time I go out of my home, with my oxygen in place, I become very short of breath and need to rest in bed the next day or two.” During my visit, at rest, her oxygen saturation was 96% with a high flow of supplemental oxygen. After a short walk, it dropped to 92% with a pulse of 110. She had already signed her DNR order. Madge did not expect to need my services yet. She would call her family physician or her respirologist for any minor problems. When she suffered a crisis causing a significant step down in her functional ability, she or her son would call me.
Fusion of the Science with the Art of Near-End-OF-Life Care:
In the next year, Madge asked me to visit twice, mainly to keep the link with me. During the first visit, she reported that was not feeling as well, though still managing her essential activities of daily living, eating for her needs, doing her crafts and small chores in her home. She had sold her car and planned to spend time at her cottage with her sons during the summer. She just wanted reassurance that her plans for the summer were realistic.
Four months later, just before Christmas, after tolerating a shopping trip for craft items quite well, on returning home she slept for a full twenty four hours, then remained in bed all day. Madge had improved but not to her usual activity. She was still managing the stairs to the basement but needed to rest about 20 seconds at each step. She was mentally very appropriate. On oxygen, her saturation level was 94%, but off oxygen for 10 minutes, it fell to 81%. Her respirologist reassessed her earlier in the month, surprised she was still alive. He felt she had progressed with increased shortness of breath but made no changes to her oxygen flow rate. Madge lived another three years.
About every six months, she had a life-threatening respiratory episode. We managed her symptoms at home. She was still clear that she would not return to the hospital. We feared each time she would not survive. She did recover each time, but never to her previous functional level.
Recurring Episodes:
Two and a half years before her death, Madge asked her son to take her shopping for craft supplies. She took a portable oxygen tank for continuous oxygen. As an extra precaution, her son brought a spare tank. While shopping her oxygen canister ran empty. She became very short of breath, sat on the floor. Several women noticed her distress and notified her son waiting nearby. He exchanged the oxygen tank and sat with her on the floor until she recovered enough to walk. Both had felt she was about to die. When she was arrived home, she stayed in her room for a week, just transferring from bed to bathroom. She recovered over the next few weeks, but she continued to have more difficulty working with her crafts.
Madge admitted, “I know I will die soon, but I have decided how to live my life. I will NOT stop doing activities even if I might die suddenly.” She was determined to do her crafts, but she was just too breathless to manage the stairs. Her son solved that problem by bringing all her craft supplies up to the living room, just a few steps from her bedroom. At complete rest, her breathing was controlled, but with just a transfer to the commode, talking, her breathing quickly became laboured. She hoped a respiratory virus was the cause, and her symptoms would improve. I was worried enough about her breathlessness that I asked the Home Care coordinator to set up shift nursing to help Madge with her essential daily activities, preserving energy for her so that she might recover enough to have a little reserve energy for her crafts. With the nurse in the home during the day, I ordered Midazolam by pump subcutaneously, a tiny continuous dose and a larger, as-needed dose, to quickly resolve a breathless episode. Madge, reluctantly, agreed.
To our surprise, slowly, Madge stabilized and then improved. Within a month, she managed walking slowly and carefully on the main floor with minor breathlessness. She adapted to the pump for Midazolam, using about six Midazolam boluses each day to recover from a walk or a trip to the bathroom. She started to sleep and eat well. During a visit, at rest her pulse was 100 and oxygen saturation was 94% on oxygen. I did not think she was ready to go out of her home or climb the stairs, but she pleaded to go downstairs to sort out her craft supplies. Her son found another ‘elegant’ solution. He and his brother sat her in a straight-back chair and lifted her up and down the stairs so she could sort out her crafts.
Madge remained precarious. She could shower and enjoy the experience if she sat down during the procedure and let the nurse wash her. We had objective evidence of fragility Madge when the nurse noticed she looked very dusky after her shower. She measured her oxygen saturation with difficulty, but eventually succeeded and found her oxygen saturation was 70%. Once Madge had rested in bed for a few minutes, her oxygen saturation returned to 94%. Her shift nurse occasionally, at the beginning of her shift, found Madge asleep in bed, with her oxygen off. Her oxygen saturation was always around 44%. She would replace the oxygen and when Madge awakened, her saturations were normal. Madge had no idea how close she had come to dying.
Two years before her death, Madge had bout of marked deterioration over several weeks. There was no definite trigger, but she was in bed most of the time and much more confused. She was breathless with a short walk to the bathroom and managed only one shower each week, totally dependent on the nurse’s help. She ate less and did only a few crafts in bed. At the family’s Christmas celebration, everyone noticed that she had much less stamina, but she rose to the occasion, then slept for the next twenty-four hours. A few weeks later, she demonstrated signs of bronchitis, treated with antibiotics. She improved enough to start walking on the main floor and restart her crafts.
Eighteen months before her death, during a heatwave and humidity in the summer, Madge had more difficulty breathing, with any activity. Even short trips to the bathroom led to severe coughing bouts. All her care was done in bed. Eventually, she agreed to use a commode at her bedside. Again, I started a course of antibiotics in case of a treatable infection. This time, there was no improvement. A month later, even a bed bath was too tiring and caused significant shortness of breath. She developed severe irritation of her nostrils due to the high oxygen flow required. I consulted with the respiratory therapist and together with Madge we tried a ‘moustache’ cannula to administer the oxygen with less irritation and a little more efficiency. And again, she stabilized and started to improve. Madge now enjoyed her bed bath, occasionally walked to the living room and spoke in long sentences. She was mostly in bed where she was still able to do her crafts.
One year before her death, her oldest beloved dog deteriorated suddenly and died within a day. Madge was distraught, causing a rapid and obvious progression of her illness, back to severe shortness of breath and coughing with any activity, taking a long time to settle. Her world was back to all care in bed. Again, I ordered a course of antibiotics which seemed to help somewhat. Within a few weeks, she tolerated transfers to the living room sitting on her walker, a bed bath every four days. Madge ate enough for her needs.
Six months before her death, her son found Madge sleeping with her oxygen off several times. Each time, she was dusky but very comfortable. He put the oxygen moustache back in place, and she recovered before awakening. During the day, she insisted to go outside on her walker to sit and do some quiet crafts almost daily. On return to bed, we could not measure her oxygen for about five minutes even though she was not breathless. When her pulse became palpable, her oxygen saturation was above 90%. She slept about four hours after each activity.
During one of my visits, when Madge was back to sleep, I spoke with her two sons. We quietly reviewed the changes observed in the last six months. When I asked their feelings about the approach to Madge’s care in the future, both understood that one day they would simply find Madge not breathing in bed or suddenly cease to breathe while sitting outside. They wanted to continue with the present regime, it was essential for Madge’s mental well-being.
Ominous Premonition:
Four months before Madge’s death, she had periods of confusion, especially at night, including hallucinations and sleepwalking. She described difficulty sleeping at night, waking up suddenly, being very confused. Her son had difficulty reorienting her. We were likely seeing the effects of Madge slipping into a Cheyne Stokes breathing pattern in her sleep, triggering her to awaken with the brainstem’s order to restart breathing. The confusion was likely due to the increase in carbon dioxide. This was a more ominous sign that her death was approaching. Madge and her family agreed that comfort and prevention of falls at night were more critical than functional ability during the day, so we decided to try Nozinan at bedtime. Madge did sleep better and felt clearer during the day, but she was too sleepy, so she refused to take the Nozinan. She did stabilize for a few weeks with a slight increase in the Midazolam bolus.
Two months before her death, another beloved dog died. She progressed, now hallucinating, and walking about most nights. After a bed bath, her oxygen saturation was 69%, recovering back to 98% after a rest. Her son agreed to try a small dose of Nozinan and Phenobarbital at night for the confusion and to help her sleep and stay in bed. It was tolerated and partially effective. She still awakened at night but did not get out of bed. For the next month, we achieved much better control of the confusion, with no further changes in the medication, likely because Madge was more tired from her illness. She was sleeping most of the day. We inserted a urinary catheter to decrease the need to transfer to the commode, now used only for bowel movements.
Madge could eat enough for her needs. She spoke softly, only able to concentrate for a few minutes. With less activity, she needed fewer boluses of Midazolam. Her oxygen saturation at rest was 92% on oxygen.
Destabilization:
One day before her death, during her care, she required frequent Midazolam boluses to maintain comfort. She settled, had a quiet evening, ate, and spoke with her son. But by the middle of the night, she started to struggle again with her shortness of breath despite several Midazolam boluses. Her son called her family to the home.
Death Imminent:
The morning of her death, Madge appeared uncomfortable, in pain, struggling with her breathing when the nurse arrived for her shift. I advised Hydromorphone and Nozinan subcutaneously. She settled within a half-hour. On my arrival, she was quiet, her respirations were irregular and gasping with minimal congestion, her limbs were mottled, and she had no radial pulse. Her heart rate ranged from 120 – 180. A few minutes later, she died quietly with her family beside her.
Timeline To Death
Predicted: Several Months Actual: 5 years
Madge’s care was complicated mainly because she was very independent and wanted to control her life and maintain her regular daily activity. Her respiratory disease was highly aggressive, her body constantly warning her to slow down. She did not listen and frequently was on the edge of the cliff, almost dying with each crisis.
These episodes continued for five years. After each significant respiratory crisis, she recovered but never to her previous functional ability.
Madge’s deterioration followed the typical pattern of patients following the erratic path toward death triggered by episodes of lung failure with an obstructive component, though a more protracted course than usual.
With the crisis over two years before she died, I had asked for shift nursing forty hours per week from her Home Care coordinator, explaining I thought she had less than three months to live. The care provided by the nurse allowed Madge to recover from each of her life-threatening crises over the next two years. Every time the home care coordinator tried to terminate the shifts, Madge would have another major respiratory crisis.
She, therefore, continued with the shift nursing. And did so repeatedly for over two years.
In part, I tell Madge’s story because it demonstrates one of the most significant weaknesses of the palliative care system for patients with a long near-end-of-life period. Madge was one of the lucky ones. She was able to have all the services she needed and a very supportive family. It continues to be one of the great difficulties for patients with a very aggressive illness, who are on the edge of death with small triggers and recover with good supportive care. The home care system is not set up to deal with these cases.
It is not the fault of the professional caregivers and coordinators. It is the system’s fault. Unfortunately, the patients and families are essentially told that their loved ones are not sick enough to have the services they need. The families caring for their loved ones know better. They say, “My mother (father or spouse, etc.) are very sick. We see them deteriorating – some days they are so very close to death. How can you say they are not sick enough – that they are not dying?” Families and patients feel abandoned. And when the final crisis occurs, it does so very rapidly, often leaving no time to restart the services.
Specific Diagnosis: Pulmonary Fibrosis
Erratic Path Toward Death Lung Trigger
Pre-referral Information:
Robert, 84, presented with three years of increasing shortness of breath triggered by activity. Investigations confirmed a diagnosis of pulmonary fibrosis and mild aortic stenosis. Over the years Robert’s respirologists treated him with short courses of Prednisone, a steroid, that consistently improved his symptoms, but shortly after the Prednisone course was completed, he would relapse. The severity of his breathlessness attacks slowly increased, and his oxygen saturations decreased to the low 80s on room air even at rest. Robert was now dependent on supplemental oxygen. He continued to be more breathless and at his last visit to a respiratory rehabilitation program, Robert’s physicians increased his oxygen flow, prescribed Prednisone daily for two weeks and referred him to community palliative care.
Initial Contact:
I first met with Robert and his wife a year before his death, three weeks after his last rehabilitation assessment. Robert understood his disease well and participated fully in the conversation. He stated that shortness of breath, as always, was his primary symptom. It had become much worse again since he developed sudden pain in his chest the week before my visit, coinciding with the end of his Prednisone course. He felt normal at rest but had no reserve to do anything but sit. Still, he could climb stairs in his home once daily, very slowly.
We reviewed his near-end-of-life goals. He wanted to stay at home and die at home. His wife was willing to care for him. But, he stated, “What I really want is to go to New Jersey for a family reunion in the summer four months from now.” In reviewing my data, this way of thinking was prevalent in patients with pulmonary fibrosis. With activity, Robert felt that his death was moments away – and he was right. But, at rest, he felt perfectly healthy and wanted to live his life his way – and again, he was right. At rest, his lungs had enough healthy alveoli to easily transfer the oxygen he needed to survive, and the rest of his essential organs were healthy enough to function well. But Robert wanted to be active, not just sit for the rest of his life.
My assessment at my first visit was that I needed to build trust with Robert. Perhaps In could achieve that goal by providing him with a period of stability that would allow at least some activity. I restarted Robert on a small dose of Prednisone, agreeing to continue it indefinitely if he found good benefit. My rationale was that pulmonary fibrosis has an autoimmune component to its relentless progression. Prednisone has anti-inflammatory effects. If the tissues about the alveoli being damaged were inflamed before scarring occurred, perhaps the anti-inflammatory effect of Prednisone would settle the swelling, improve the absorption of oxygen and, therefore, the quality of his life. Robert always liked his Prednisone, so he was pleased to try the new approach.
The Fusion of the Science with the Art of Near-End-Of-Life Care:
Robert felt no better, but his wife noticed he was doing more and eating better. He was still breathless on short walks. I observed him walking and noticed he tended to hyperventilate when beginning to feel breathless. If I distracted him, he quickly improved with normal oxygen saturations. He could speak in long sentences without taking a breath. I reassured him and his wife that his subjective breathlessness was not life-threatening. But he was worried, and that worry was making him hyperventilate, leading to more breathlessness – essentially a vicious cycle. I offered him an oximeter to measure his oxygen saturations so he and his wife could objectively determine the seriousness of a breathless episode. I also demonstrated a series of breathing exercises. Robert continued to improve and now believed that he was better. He went out by himself occasionally, enjoying lunches with his buddies. He slept very well. Even when he was short of breath, when he noticed that his oxygen saturation was 97% on oxygen, he relaxed. On my examination, his breathing was much better, and his mentation was clear. Robert was feeling so well that he thought he might ask his respirologist for a second opinion. He no longer felt that he had pulmonary fibrosis.
Robert had no exacerbations of breathlessness for two months, so he started to plan his family reunion trip to New Jersey in two months in the future. As a trial for the New Jersey trip, Robert, feeling exceptionally well, drove with his wife to Montreal for lunch with his family. He tolerated the trip very well, using his oximeter to reassure himself that his oxygen saturation and pulse remained normal. Two months later, Robert and his wife had a great trip to New Jersey. On arrival, he was apprehensive because of the high temperatures and humidity, but his relative’s home had air conditioning with a pool in the backyard. On his return home, he was just fatigued and rested most of the following week.
Premonition:
In the next four months, we started to see premonition moments, observations that more of his alveolar walls were fibrosed. Robert had much less response to the Prednisone and his ‘world’ slowly became progressively smaller. After the trip to New Jersey Robert admitted to more fatigue with activities. After walking to the bathroom, he measured his oxygen saturation at 75%. Within 5 minutes of rest, his oxygen saturation recovered to 93%. Still, his mentation remained clear. Robert asked for a walker to continue his outside walks. He was still driving, although only for very short distances. I advised against doing so. We talked again about pacing his activities and preserving his energy for essential activities. Then, Robert started to use his walker in his home, managing stairs slowly once a day, doing his essential activities more slowly, requiring more rest to recover. We talked again about preserving his energy and this time he listened. He set up a chairlift for his stairs and he used his walker all the time. Robert stopped driving. With his small reserve of energy, occasionally, he was able to go out for a meal, driven by his friends, and recover quickly. A few months later, he had a wonderful Christmas celebration with his family, his vital signs remaining stable throughout.
Two months before his death, Robert started to have more difficulty with any activity, including talking on the telephone. He did continue to eat and drink well. He slept well most of the time, occasionally using Lorazepam. He frequently had breathless episodes, then suddenly hyperventilating even at rest. Robert recognized the changes and agreed readily to more help. I knew he tolerated Lorazepam well, but it caused too much drowsiness during the day. He agreed to a trial of Midazolam subcutaneously to control these episodes. It was effective if he took a dose – which he rarely did.
One month before his death, Robert was more breathless on any activity, even shaving. He continued to eat well, and his vital signs were normal at rest on oxygen. His wife was very worried about falls when he went from bed to the bathroom. We had a discussion with Robert about a bedside commode and a urinal. He respectively declined.
Two weeks before his death, Robert’s breathlessness was more severe, and his recovery took longer. Surprisingly to his wife and I, he willingly accepted help with walking and transfers. He never thought to ask for the Midazolam injection when breathless. Now that he had assistance with transfers and walking, I asked him to start the Midazolam by pump, with a low continuous rate and a bolus dose for his breathless episodes. The nurse or his wife could hold the pump for him during transfers and ambulation. He agreed.
Destabilization:
Two days before his death, Robert reported severe pain deep to his scapula, worse with breathing and coughing, but not with movement. It was like the pain he experienced before just before I started to care for him. He felt the Midazolam was ineffective. He appeared in pain. His pulse was 76, his breathing was shallow but not distressed with an oxygen saturation of 91%. For the first time his thinking was a little slow. He had Hydromorphone tablets in his home that he had never taken. I suggested he take one dose during my visit. He settled well, without drowsiness. I told him he could use the Hydromorphone up to four times a day for his pain if he wished. The next morning, I called his wife. Robert had a good night. He awakened in the morning in pain but was reluctant to take Hydromorphone. When he was persuaded, the medication was beneficial.
Death Imminent:
On the evening of his death, after a quiet day, with his pain in reasonable control, Robert made three trips, in quick succession, to the bathroom just before midnight to try to pass urine. On the third try, he was successful. On returning to his bed, he suddenly became very breathless. Robert sat at the side of his bed, rested his head on his walker before transferring into bed with his wife supporting him. Suddenly, he fainted, fell slowly to the floor, and did not restart to breathe.
Robert’s progression was very characteristic of patients diagnosed with pulmonary fibrosis. His healthy air sacs functioned efficiently but his scarred air sacs did not function at all. His alveoli being attacked through the auto-immune process responded well to small doses of Prednisone for months, until they became scarred.
Robert’s symptoms were very characteristic as well. At rest, he felt perfectly well, but after activity, overextending his lungs’ ability to compensate with extra oxygen, he felt his death was imminent. As more and more alveoli scarred and his functional lung capacity diminished slowly but relentlessly, his world became smaller and smaller.
On the evening of his death, Robert did an unusual amount of activity by going the bathroom three times in quick succession, not allowing himself to recover after each attempt. His need to pass urine was so strong that he did not heed his body’s signal that he should stop walking. He overextended his lungs. Robert could not recover from that last trip – and died suddenly unable to provide oxygen to his brainstem.
Of my patients with pulmonary fibrosis 50% died suddenly after a similar scenario.
Specific Diagnosis: Respiratory ALS
Erratic Path Toward Death Lung Trigger
Pre-referral Information:
Diane was diagnosed with ALS just before her 50th birthday. I became involved in her care five years later. Through the progression of her disease, Diane and her husband had managed their activities of daily living and family life with remarkable resilience. As her disease progressed, they found innovative ways to renovate the bedroom and bathroom to allow easy wheelchair access and cope with the increasing physical limitations caused by her illness. Diane remained very much in control of the household affairs and planned all the family reunions for birthdays, holidays, etc. During that period, her greatest joy was her granddaughter, Cleo, born three years after her diagnosis of ALS. Their love for each other was palpable when I observed their interactions during my visits.
Diane had researched ALS and understood her illness, the likely progression, and the symptoms she would be facing. She was determined to fight against her limitations and live her life to the fullest. She had been assessed routinely by the ALS clinic and provided with mobility equipment for progressive physical weakness as well as a BiPAP and suction machine to assist her breathing and clear her secretions. She had asked to be followed by palliative care about two years before I met her. A community palliative physician had accepted the referral, had visited her for symptom control, prescribed various medications for her shortness of breath, anxiety, secretions, and pain, and then delegated ongoing home visits to her nurses.
Diane’s need for a community physician who would visit her at home became imperative when she could no longer leave her home to visit the ALS clinic. She wanted to live as long as possible to enjoy her family. Diane wanted explanations and, also, to participate in decision-making regarding the approach to her care and the security that a physician would be available to her in case of emergency. Her goal was to stay at home until her death. Routine physician home visits were difficult in Ottawa at the time. Diane lived in the extreme east end of Ottawa, making the trip to her home time-consuming.
Diane had heard from staff at the ALS clinic and the ALS Society that I was willing to provide care for patients with ALS early in the course of their illness as soon as they were ready to discuss and take a palliative approach to their care at home. She asked me to visit to understand if I could help her in any way.
Initial Contact:
I set up my first visit with Diane, her husband, and her regular personal caregiver. Just entering Diane’s home, I could observe how well Diane and her husband had organized their home for her care. It was apparent, as well, the obstacles confronting Diane and her husband in the present and the difficulties to be overcome in the future. Diane was not in the early phase of her illness. She was either confined to bed or mobile in an electric wheelchair. She could only communicate with the blinking of her eyes, some small facial movements and expressive eyes that indicated her pleasure, anger, indifference, or the need for more information.
Diane and her caregiver had prepared a list of questions for my attention. The first visit was long. Her husband and caregiver were able to explain details of the progression of her illness, the current issues and the medications that had been prescribed to address her ongoing symptoms. I listened carefully while observing Diane’s reactions and thinking about her limitations. I tried to understand what I could do for her, and, more importantly, what she would let me do for her.
Shortness of breath was one of two most distressing symptoms. Diane was breathless at rest. She had required assistance for breathing with BiPAP for a few years at night but now required the BiPAP up to fourteen hours daily. Her vital signs were normal with a pulse at 88 and oxygen saturation of 96%. Diane continued to sit in her wheelchair throughout the visit, participating fully. She had a reasonable effort of breathing, but it became more laboured as she tired. Diane indicated clearly that she wanted to be alert, did not wish to be tied to the BiPAP during the day, and wanted to keep her daily routine as normal as possible, including a daily shower. Diane was tolerating her BiPAP. She had a pressure pad on her pillow that she could activate with a slight turn of her head to call her husband through the night if she felt short of breath or had difficulty with the BiPAP. She had caregivers each morning and evening for her care. She had the care she needed for now. It was apparent, though, that she was very fearful of any further loss of independence.
Still, we would need to make changes in the future. Diane would need a shift nurse in the night to be with her in case of distress with her breathing and problems with the BiPAP, urination, or bowels.
She would need a mechanical lift to transfer from her bed to her wheelchair to continue to shower, and medications to control the fear of breathlessness – perhaps Nozinan initially, then later Midazolam, and Scopolamine. At the present moment, I needed to recognize that she and her husband were doing an amazing job in their approach to Diane’s care. I just needed to monitor.
The second most distressing symptom was a build-up of copious secretions in her throat requiring frequent suctioning during the day. Fortunately, she did not have many secretions in the night. She had reported this symptom to all her physicians. They had prescribed ‘drying’ medications – Amitriptyline and Atropine drops. Diane used only small doses to minimize the drowsiness of all this group of medications. I observed her caregiver and husband frequently suctioning her mouth and throat as the secretions caused her distress during the visit. The secretions were not under control. I was confident that we could reduce Diane’s secretions without using medications if we decreased her feeds and fluid intake. I was also sure that Diane would not be open to my suggestions. Diane believed that ‘lots of good calories would help in her energy level, and lots of fluid would help her bowel function’. How could I explain to her, on this first visit, that I wanted her to decrease her food and fluid intake? I realized that I could not. Therefore, I put the issue on my list of problems to be addressed in the future.
Diane had anxiety, expressed by disturbance of her sleep/wake cycle and occasional panic attacks related to the increased secretions and breathlessness. Clonazepam seemed to be the best to help keep her calm. She liked its benefits, using it three times daily without being drowsy. Occasionally she used Nozinan tablets for the double effect of drying her secretions and reducing her anxiety at night, but found it caused too much drowsiness. The doses of Clonazepam and Nozinan were the smallest available tablets.
There was no need for intervention at present, she was sleeping well – all the better because Diane would not have accepted any intervention likely to increase her drowsiness. In the future, this symptom, related to her secretions and increased shortness of breath, would be the most critical symptom to control.
Nutrition was very important for Diane. She was tolerating her feeds well without nausea. Her dietitian encouraged 4-5 cans of meal replacement daily supplemented with protein powder. Diane trusted her dietitian, believing that the best nutritional regime would give her the energy to fight the illness and regain some strength.
Pain was a constant problem. Diane had two types of pain, a burning sensation in her legs and muscle spasms. Both had recently progressed in severity and frequency. She was reluctant to take Morphine because of drowsiness but it was available in her home.
She used a muscle relaxant three times daily, regularly through the gastric tube, and occasionally Ibuprofen. I did not need to intervene in her pain control for now. Diane already had the tools to help control her pain, but she was fearful the side effects would outweigh the benefits.
I needed to develop Diane’s trust before I could make any beneficial interventions. I wondered how I could demonstrate to Diane that I heard and understood her problems and if there any intervention I could make to address some of her symptoms. I needed to use my knowledge of the science underlying her symptoms, but add to that, the art of caring for my new patient with ALS that I had learned from my experiences. Diane had been closely followed by the ALS clinic and a palliative outreach team in the years living with ALS. On reviewing her symptoms, the approach they took, the medications they prescribed and Diane’s description of her ongoing issues and goals, I felt Diane was challenging me. I heard:
I realized there was no new intervention I could suggest on this the visit. I needed to take the Family Medicine approach to her care. Diane already had the best ‘tools’ available. Now she needed ongoing surveillance, someone to talk to about the problems, how to use the tools in the best way possible. I needed to develop our doctor-patient trust. I did believe that Diane’s condition was precarious. She was already on the BiPAP fourteen hours a day and her great difficulties with secretions made her prone to aspiration pneumonia.
I proposed to visit every two weeks for the first few months and then re-evaluate. Together we decided the best timing would be Saturday morning after her morning care. I would have no scheduled visits with my other patients. Her most experienced personal caregiver and her husband would be present to help with communication. Although I asked Diane to prepare a list of her concerns for each visit, it still took time to discuss them. I needed to prove to Diane that I would take the time to listen to her concerns.
Drawing on my expertise in caring for patients with ALS, I assessed that Diane might have a prognosis of a few months.
I would have time to better understand her individual needs and the family dynamics and learn how to best approach her symptoms. I felt I would be able to continue this regime of home visits for the next few months without compromising the care of my other patients. Diane proved me wrong. Indeed, she did have a fighting spirit fueled in large part by a grandmother’s love. Diane survived for just over two years after I met her.
Fusion of the Science with the Art of Near-End-of-Life Care:
During the first year I took on my observer role, essentially building trust for the future. I occasionally made a few suggestions but did not expect Diane would act on them. I visited when Diane requested. I was always available by phone. Diane remained amazingly stable. I tried to give control back to Diane and her family by observing her strengths and emphasizing them by looking for gaps in knowledge and educating; and by looking for her greatest fears and trying to alleviate them. I knew Diane and her family were the experts in this situation, and I would use their expertise in helping make decisions with them.
I asked Diane and her family if I could explain the science of this disease. They were pleased to learn. I reviewed the hierarchy of the body and explained the body’s natural path toward death. Then, I added the unique complications caused by the progression of ALS, explaining it was disease of the peripheral nerves, expressed by weakening muscles in varying degrees while the organs essential for survival remained normal. Then, I individualized the ALS process unique to Diane. At this stage of her illness, Diane had two groups of affected muscles that were starting to cause life-threatening complications, her thoracic muscles necessary for breathing, and her bulbar muscles, making swallowing difficult and increasing the chance of aspiration even though all her feeds were through the gastric tube. I then explained my objective tools for evaluation at each visit, trying to anticipate and prevent an impending crisis by reviewing: Diane’s functional ability; her heart rate and pulse strength; her oxygen saturations at the fingertips; her breathing patterns and dependency on the BiPAP; and the frequency of medications needed to control her anxiety.
Although Diane remained at a stable functional ability in the first six months, she was fragile with good and bad days. The most distressing symptoms remained the secretions in her throat and the fear of choking. Diane remained in control, and although we had discussions about her symptoms, she would not let me make any changes except to agree to take Nozinan a little more regularly at bedtime. Towards the end of the first year, Diane and her family observed increased effort required to perform any activity, but Diane kept to her routine. She did agree to nursing shifts for the nights. This additional help for her care also allowed her husband to sleep well
Towards the end of the first year, Diane started to request weekly visits. She wanted to explain her concerns and better understand the significance of her worsening symptoms. I used this opportunity to continue to explain the science of progression of this disease with her. First, she wondered about her rapid pulse, frequently up to 110 after an activity and subjectively she was more tired and felt more air hunger off the BiPAP. I explained that her heart rate at 110 was not dangerous. Still, it was an objective sign of the body’s compensation. When her body had more difficulty getting enough oxygen for its needs, signals were sent to her heart to beat more powerfully. As her heart tired, it could only beat faster and less efficiently. The increased fatigue and air hunger were subjective signs of the same problem. Her body was trying to save as much energy as possible for essential functions. Her body was warning Diane to pace her activity to prevent a crisis. Over time, there would be more urgent signs demanding her to stay longer on the BiPAP, eat less and increase her sleep. If anxiety were a significant symptom, we could add extra Clonazepam or Nozinan for comfort, maximize rest to give her body time for essential functions. Her body would then present her with a ‘package’ of energy to do her non-essential quality-of-life activities. And as the disease progressed, she would start to retain carbon dioxide causing her to sleep more and more, still comfortable on the BiPAP. Whether on or off the BiPAP, her death would come in sleep.
Second, Diane was concerned about using the BiPAP and Clonazepam as ‘crutches’ when having a panic attack, stating, “Maybe I should be strong and not depend on them?” I explained that when anyone becomes anxious, there is a tendency to hyperventilate, causing the breathing muscles to tire quickly, leading to more air hunger and anxiety. The medication and BiPAP were ‘tools,’ not ‘crutches’ to help regain control. Sometimes, knowing that the BiPAP and Clonazepam were available allowed the patient to control the panicky feelings without resorting to the tools. Still, it would be important for Diane to follow her body’s messages.
Diane listened carefully to my explanations, my suggestions of decreasing fluids, decreasing the feeds just a little, and increasing her anti-anxiety medication. Of course, she needed time to think. She agreed to only minor changes, taking Nozinan more regularly at bedtime. But then, when she was tired, she blamed the Nozinan, so would stop it for a few days. She was always comfortable taking an extra Clonazepam for her anxiety. And then, to my surprise, near the end of that first year, she spontaneously decided to a trial of decreasing her feeds by a can daily, providing she could continue to have her regular coffee. She was pleasantly surprised when she experienced much less difficulty with secretions without increased fatigue for the next few months.
Premonitions:
One year before Diane’s death, premonition signs became evident. During her very important daily morning routine, including her shower, symptoms of shortness of breath, secretions and panic increased markedly. Understanding the importance of this routine, I suggested that the night nurse could give her an injection of Midazolam, a minor tranquillizer, before and after to decrease her shortness of breath, but short acting so that she would not be sleepy after she recovered from the activity. She agreed and it made such a difference! Diane was amazed! She felt stronger, remained calm and had no hangover effect after a short rest. Diane, herself, asked permission to take the Midazolam whenever she was panicky during the day. Because there were no nurses through the day, we administered the Midazolam via a pump. She liked it so much that she substituted the Midazolam for her Clonazepam.
Diane had a few months of increased control of her symptoms with an increased ability to do her desired activities. But Diane’s disease progression was unrelenting. Not only did we need to control her anxiety, but we also needed to do more to preserve her energy. Diane was clear that she needed her shower every day and transfer to the commode for bowel movements, but she did agree to a urinary catheter, and to a mechanical lift for her transfers by nurses and caregivers to save energy. Still, when her husband was home, she preferred to be lifted by him as he had always done.
Diane’s nights were difficult. She started to awaken frequently. The Midazolam was not enough for her to sleep well. Her vital signs on and off the BiPAP and after activity remained in the normal range. I suggested doubling the Nozinan and restarting her bedtime dose of Clonazepam (both were longer acting than the Midazolam). I also advised to add a small dose of Phenobarbital at bedtime, attempting to avoid sleepiness in the day, but as an aid to sleep and control her nerve pain. Diane benefitted from these changes for a few months. Then, with Diane’s permission, we held a family meeting to explain the changes, discuss her future needs and reaffirm that she wished to be home.
As Diane started to trust me, she dared to ask me about her secretions, “Why do I have so much saliva in my mouth and throat?” I explained that with less physical activity, the body needed much less food and fluid intake. As the body weakened, it was directed to preserve energy processing food and fluids only for its essential needs. Any excess intake was eliminated leading to secretions, regurgitation, cramps and diarrhea. Diane was now open to making changes. We reduced her feeds by half. Diane suggested an increase in Midazolam to help with activity during the day and Phenobarbital in the night to help her sleep, an increase in shift nursing and freedom to ask for extra Nozinan. Diane asked me to visit twice weekly.
Six months before her death, Diane remained reasonably comfortable for a few months after our changes. She maintained her functional ability with only a few more hours on the BiPAP, now eighteen hours through the day and night. Her vital signs remained normal. Then, slowly she started to feel some breathlessness while still on the BiPAP, especially in the early morning hours. We added a small extra dose of Phenobarbital at about four am. Her daily shower was still a must! I discussed using a small amount of Hydromorphone to help with the sensation of breathlessness while on the BiPAP. I explained that the feeling of breathlessness was subjective, not dangerous because her oxygen saturation and heart rate were normal. As usual, I left the decision to Diane but wrote an order for Hydromorphone every four hours upon Diane’s request through the gastric tube. We briefly discussed the need to limit her transfers soon and decrease the feeds further, but we made no decisions.
Diane thought about our discussion about limiting transfers until my next visit. She composed a note with her nurse to clearly express her wishes, stating:
On reading the note, her husband refused ever to remove the BiPAP – he would feel he had played a role in killing her.
I acknowledged her wishes and frustrations. But I knew we could not come to a compromise during the visit. The nurses and I knew we needed to continue the daily routine until circumstances made it impossible to continue the transfers and I promised Diane we would continue her daily routine. I reassured Diane that the BiPAP would not keep her alive for a long time when the disease was so advanced that the essential organs were failing. For now, we would observe for changes visit by visit.
Ominous Premonition:
Over the next few months, Diane had several sudden episodes of shortness of breath, quickly controlled with medication. But Diane was still reluctant to take preventative drugs to promote better sleep, or to decrease her feeds and fluids to save energy for her during the day. Then, one day on her own, she asked to take Hydromorphone at bedtime and decrease her feeds and fluids. She benefited from the changes almost immediately with less leg swelling and fewer and more easily controlled secretions. She slept well at night and tolerated her morning routine much better. She was so pleased that she initially decided to continue the new regime. Then, of course, when she had no severe symptoms, she felt her fatigue more. Blaming the medications for her fatigue, she tried to go off the regime a few times as a test, resulting return of her distressing symptoms.
Diane was on BiPAP most of the time now except for her transfers. Eventually, she needed the BiPAP to continue her showers and enjoy them. She maintained her routine for another two months without significant complications. Overall, all caregivers noticed more lethargy and less ability to communicate. Her pulse was 80 and oxygen saturation 95% on BiPAP. We observed that she had minimal chest expansion on the BiPAP using only her diaphragm and accessory muscles.
Life-Threatening Premonition:
Two months before her death, Diane demonstrated even more severe premonition signs of progression with increasing fatigue, sleeping for a few hours after her shower and at least four hours in the afternoon. Her daily shower was exhausting but, for her, essential. Still, she had no severe episodes of secretions, and her vital signs remained normal. Diane’s response to the increasing fatigue was, “It must be the medications.” But she did not ask to decrease the regime. Very significantly, before Christmas, she asked to stop the feeds altogether. She wanted to keep just her coffee and clear fluids. Within a few days, she felt ‘so’ much better. She was breathing easily with fewer secretions. But her family thought she was giving up and asked her to restart some of the feeds. She agreed since she wanted to please her family and to be the best possible for Christmas. Diane tolerated the Christmas celebrations, mostly in bed. She was not too tired to communicate efficiently, stating that the medications were effective and that she was thinking of decreasing the feeds again. She was not ready to increase the Hydromorphone to help with the shower.
One month before her death, Diane was weaker but still in control. She was still trying to experiment a little with feeds and medications. She restarted Hydromorphone by injection at bedtime and shower time. She had much better comfort and fewer secretions. And again, because she was feeling so well, she decided she should try a little meal replacement maybe to regain some energy. Immediately she had more secretions, and she stopped again.
Destabilization:
A few days later, we observed the most dramatic change yet, the first objective signs of destabilization. She was difficult to awaken in the morning. Finally, she awakened enough to shower, then fell asleep immediately until the evening. Her vital signs were still in her usual range and there was no increase in her secretions. She did improve the next day, enough to state, “I will no longer take the meal replacement but please keep the coffee.” When questioned, Diane seemed pleased with the decision, indicating she had fewer secretions and was more comfortable.
A few days later, she was awake and well enough to participate fully in her darling granddaughter’s fourth birthday. Diane’s husband came to me at the end of one of my visits during that period. He showed me two photographs of Diane, one when she had been encouraged by the family to restart the meal replacement at Christmas and one at Cleo’s fourth birthday party when she had stopped the feeds. He pointed out how uncomfortable Diane appeared when on the meal replacement and how radiant she appeared off the food. He stated, “What I have always wanted was to see Diane comfortable. It is ok for her to stop her feeds.”
Soon after, Diane communicated clearly that she was still satisfied with her decisions. For the first time, she asked, “How long?” I explained that she would not starve to death. Whenever we decreased stress on her body, she had a plateau in the past. I believed this time it would not be long-lived, perhaps a few weeks. We would make sure she would remain comfortable.
Death Imminent:
Eleven days before Diane’s death, the nurse and Diane’s husband reported that she had had a quiet night and appeared comfortable. But, with the removal of her BiPAP for three minutes for mouth care, she had become very dusky, her oxygen saturations quickly dropping to 78%. She settled immediately with the BiPAP in place. The following morning, she was transferred to her wheelchair for the usual morning routine care but remained unresponsive. After personal care and mouth care, her oxygen saturation dropped to 73%. I ordered Hydromorphone subcutaneously and to keep her in bed. She recovered slowly and comfortably over the next few hours. But she would no longer respond to questions, never re-opening her eyes. From my perspective, she made my decision very easy. She did not ask to remove her BiPAP before she closed her eyes, trusting her husband and caregivers to make her care decisions.
I felt she was now at the end stage of her disease with desaturations whenever she was off the BiPAP or during her transfers even with a lift. After discussing with Diane’s husband, we stopped all the gastric tube feeds, fluids (except for a little of Diane’s beloved coffee!), and her medications . I kept the Midazolam unchanged and increased the Phenobarbital to twice daily intramuscularly. I started Hydromorphone (one vial) and Scopolamine (one vial) every four hours regularly subcutaneously. The nursing was increased to twenty-four hours a day. All the nurses knew Diane and renewed their efforts to give Diane the best care possible. All made sure her hygiene was up to her standard with her hair and make-up just right, knowing how important that was for Diane.
Diane lived for ten days. Her family agreed with the approach to her care. Diane remained peaceful and quiet with no congestion. Her family all wished comfort only agreeing that if Diane suddenly changed but remained comfortable, no measures would be taken to prolong her life. No one asked to have the BiPAP removed. All agreed to let Diane tell us in her way when she was ready. Diane’s husband was now a ‘husband,’ not a caregiver. He expressed to me, “I have not seen Diane so peaceful and so free of congestion for years. I can now let her go whenever she is ready.”
Timeline To Death
Predicted: Few months Actual: 2 years
Diane was such a fighter. She coped day after day, fighting against this unrelenting disease – living her life her way despite losing more and more control. When I met her, even though she could only communicate with her eyes, she made sure I knew that she was still mentally clear. She knew exactly what was going on in her home and in her illness. With all the information, she made her own decisions.
She lived longer than anyone ever expected. The love for Cleo, her granddaughter, played a huge role. Cleo saw Diane as the grandmother she loved. The day after Cleo’s fourth birthday, Diane no longer had the strength to take a shower. She did not make demands of her caregivers. She trusted that they would take care of her – and they did. She gave her husband the ultimate gift – she did not ask to remove the BiPAP. Diane allowed her husband, who had cared for her through her entire illness, to achieve his goal, “I just wanted her to be comfortable. She has been so peaceful with no secretions for the last ten days. Now I can let her go.”
Diane’s approach to her symptom control was very difficult for her nurses and physicians. We thought we could help her be more comfortable through her illness. Yes, she wanted to be comfortable, but far more important, she tried to live and be as functionally and as mentally clear as possible. So, she often chose to suffer from her secretions, breathlessness, and pain to achieve her goals.
Even though it took her a long time to agree to any interventions, she still wanted the link with her physician and her nurses even if ‘her’ way led to crises. Diane wanted so much to die at home.
I knew on the first visit that I would need a spectrum of injectable medications and reduction of her feeds to control Diane’s severe symptoms. I also knew that Diane would not believe in my plan with the medications and feeds until much later. Symptom control for Diane would take great patience on my part. I understood the science of symptom control, but Diane taught me the art of symptom control – a different approach for each unique patient.
Diane closed her eyes after Cleo’s birthday without giving her usual care directives nor telling her husband to remove the BiPAP. This action spoke volumes to her husband, family and caregivers. This permitted me to keep her comfortable, allowed the nurses to do continue her care and gave her family great peace. She died quietly ten days later.
Diane was the center of the care. She forced all her caregivers to let her live her life her way, in control of every decision. Throughout the two years, I had the privilege to care for Diane, and she gave me an intensive course in how to care for patients with ALS. I have used her experience to help so many other patients. When I asked her if I could describe her journey in a book, to teach others, she was amazed and readily agreed, pleased to help others.